Wellcare Provider Appeal Form
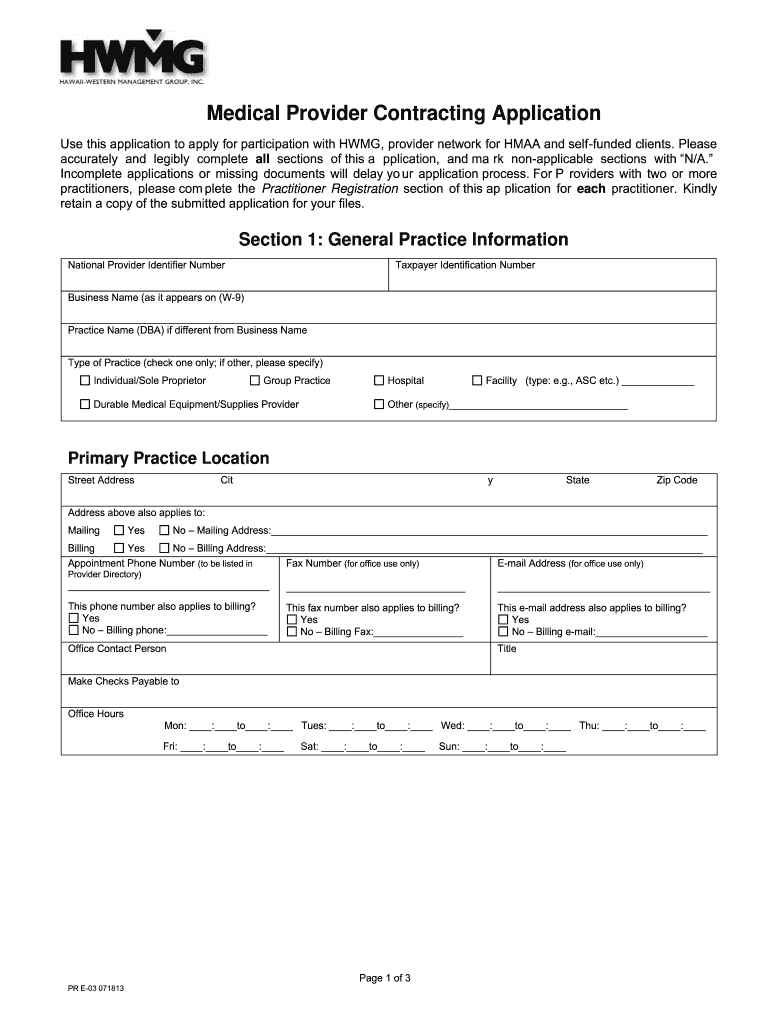
Wellcare Provider Appeal Form - Is a communication from the provider about a disagreement with a claim dispute (level ii) request for reconsideration. All fields are required information: Web detox and substance abuse service request. Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Web providers can complete the provider dispute resolution request, available in the provider library at. We have redesigned our website. Appeals should be addressed to: Forms and references, when submitting an appeal. Address for provider disputes and appeals. To access the form, please pick your state:
What is the procedure for filing an appeal? All fields are required information a request for reconsideration (level i) the manner in which a claim was processed. To access the form, please pick your state: Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Web provider payment dispute. Web providers can complete the provider dispute resolution request, available in the provider library at. Appeals should be addressed to: A request for reconsideration (level i) is a communication from the provider about a disagreement on how a claim was processed. Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Appeals 4205 philips farm road, suite 100 columbia, mo 65201.
A request for reconsideration (level i) is a communication from the provider about a disagreement on how a claim was processed. Send this form with all pertinent medical documentation to support the request to wellcare health plans, inc. How long do i have to submit an appeal? Web if you provide services such as primary care, specialist care, mental health, substance abuse and more, please download and complete the forms below: Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. We have redesigned our website. What is the procedure for filing an appeal? Web provider payment dispute. You can now quickly request an appeal for your drug coverage through the request for redetermination form. Address for provider disputes and appeals.

Fill Free fillable Sunshine Health PDF forms
Send this form with all pertinent medical documentation to support the request to wellcare health plans, inc. A request for reconsideration (level i) is a communication from the provider about a disagreement on how a claim was processed. Web provider payment dispute. Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process..
Credentialing Application Template Fill Out and Sign Printable PDF
A request for reconsideration (level i) is a communication from the provider about a disagreement on how a claim was processed. Appeals 4205 philips farm road, suite 100 columbia, mo 65201. All fields are required information: Provider waiver of liability (wol) download. Missouri care health plan attn:
WELLCARE HEALTH PLANS, INC. FORM 8K EX99.2 PRESENTATION DATED
Address for provider disputes and appeals. We have redesigned our website. Providers may file a written appeal with the missouri care complaints and appeals department. All fields are required information a request for reconsideration (level i) the manner in which a claim was processed. Web detox and substance abuse service request.
Wellcare Forms For Prior Authorization Fill Out and Sign Printable
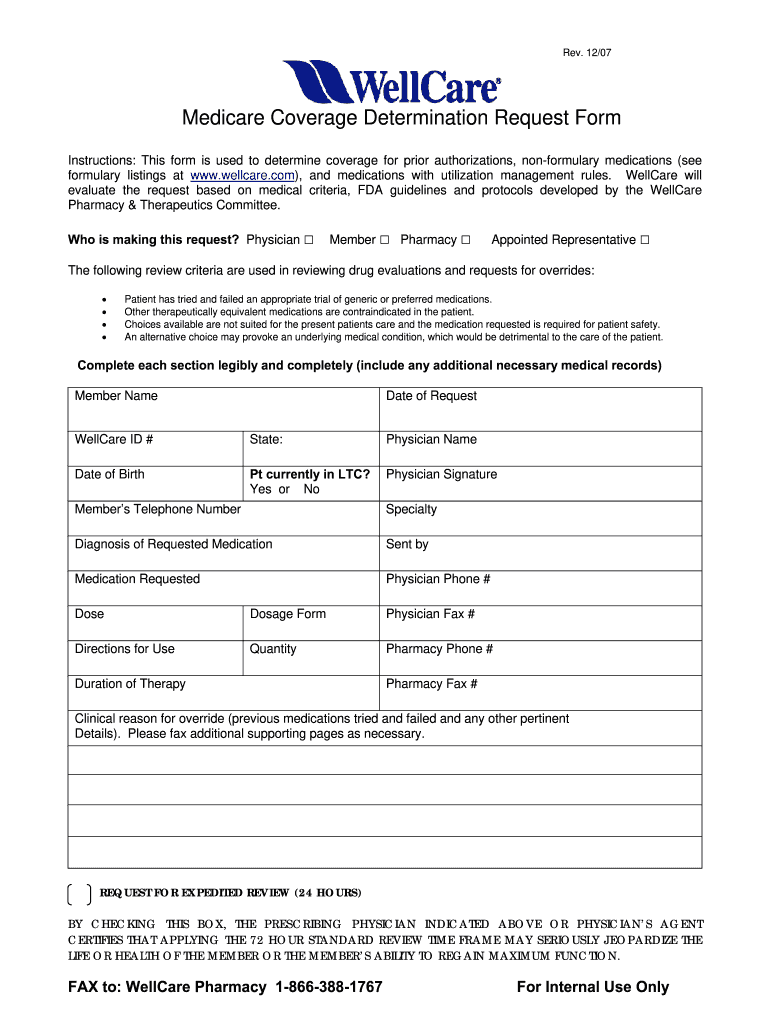
We have redesigned our website. What is the procedure for filing an appeal? Web request for redetermination of medicare prescription drug denial (appeal) (pdf) this form may be sent to us by mail or fax: Appeals should be addressed to: Web provider payment dispute.
Wellcare Value Script Enrollment Form Form Resume Examples EZVgRlkYJk
Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Missouri care health plan attn: Providers may file a written appeal with the missouri care complaints and appeals department. A request for reconsideration (level i) is a communication from the provider about a disagreement on how a claim was processed. Address for.

WellCare Provider Portal YouTube
We have redesigned our website. Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Forms and references, when submitting an appeal. Web detox and substance abuse service request. All fields are required information a request for reconsideration (level i) the manner in which a claim was processed.
Free Wellcare Prior Prescription (Rx) Authorization Form PDF
Web providers can complete the provider dispute resolution request, available in the provider library at. Web request for redetermination of medicare prescription drug denial (appeal) (pdf) this form may be sent to us by mail or fax: Is a communication from the provider about a disagreement with a claim dispute (level ii) request for reconsideration. Web use this form as.
Wellcare Appeal Form Fill Out and Sign Printable PDF Template signNow
A request for reconsideration (level i) is a communication from the provider about a disagreement on how a claim was processed. Provider waiver of liability (wol) download. Web if you provide services such as primary care, specialist care, mental health, substance abuse and more, please download and complete the forms below: Is a communication from the provider about a disagreement.

Wellcare MA/PDP Toolkit Senior Marketing Specialists
How long do i have to submit an appeal? Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. You can now quickly request an appeal for your drug coverage through the request for redetermination form. A request for reconsideration (level i) is a communication from the provider about a disagreement on.

Wellcare Card 1 newacropol
What is the procedure for filing an appeal? Web provider payment dispute. Provider waiver of liability (wol) download. Appeals should be addressed to: You can now quickly request an appeal for your drug coverage through the request for redetermination form.
How Long Do I Have To Submit An Appeal?
Missouri care health plan attn: Address for provider disputes and appeals. Web if you provide services such as primary care, specialist care, mental health, substance abuse and more, please download and complete the forms below: What is the procedure for filing an appeal?
A Request For Reconsideration (Level I) Is A Communication From The Provider About A Disagreement On How A Claim Was Processed.
Appeals 4205 philips farm road, suite 100 columbia, mo 65201. Web providers can complete the provider dispute resolution request, available in the provider library at. Provider waiver of liability (wol) download. To access the form, please pick your state:
Web Provider Payment Dispute.
We have redesigned our website. Web request for redetermination of medicare prescription drug denial (appeal) (pdf) this form may be sent to us by mail or fax: All fields are required information: Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process.
All Fields Are Required Information A Request For Reconsideration (Level I) The Manner In Which A Claim Was Processed.
Web detox and substance abuse service request. Forms and references, when submitting an appeal. Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Send this form with all pertinent medical documentation to support the request to wellcare health plans, inc.