Skyrizi Enrollment Form Printable
Skyrizi Enrollment Form Printable - Skyrizi is indicated for the treatment of active psoriatic arthritis in adults. Web download and fill out the skyrizi complete enrollment and prescription form with your patient. Skyrizi is indicated for the treatment of moderate to severe plaque psoriasis in adults who are candidates for systemic therapy or phototherapy. You must also provide a separate signature and date for hipaa authorization. 1 / / / / After submitting the form via fax, your patient will receive a call from a nurse ambassador.* you may also complete the pharmacy prescription form and fax it to your patient's specialty pharmacy. Provide your consent for eligibility determination by checking the boxes in section 5 and confirm your understanding of the terms of participation by providing your signature and date. This fax may contain medical information that is privileged and. Web use this checklist from skyrizi complete to start and stay on track with your prescribed treatment plan. Web enrolling your patients in skyrizi complete will provide your patients the support to start and stay on track with their prescribed treatment, including the resources below.
You must also provide a separate signature and date for hipaa authorization. Web print and complete the enrollment form on page 4. 1 / / / / If approved, we will ship the medication to the patient’s home unless otherwise indicated on the application. After submitting the form via fax, your patient will receive a call from a nurse ambassador.* you may also complete the pharmacy prescription form and fax it to your patient's specialty pharmacy. Once enrolled, you can expect a call from your nurse ambassador within. Web use this checklist from skyrizi complete to start and stay on track with your prescribed treatment plan. Skyrizi is indicated for the treatment of moderate to severe plaque psoriasis in adults who are candidates for systemic therapy or phototherapy. Web enrolling your patients in skyrizi complete will provide your patients the support to start and stay on track with their prescribed treatment, including the resources below. 1.866.skyrizi (1.866.759.7494) to join today.
Help with access & treatment affordability access & savings empower patients nurse ambassadors* insurance support when needed access specialists After submitting the form via fax, your patient will receive a call from a nurse ambassador.* you may also complete the pharmacy prescription form and fax it to your patient's specialty pharmacy. Skyrizi is indicated for the treatment of moderate to severe plaque psoriasis in adults who are candidates for systemic therapy or phototherapy. Web download and fill out the skyrizi complete enrollment and prescription form with your patient. Priority partners 7231 parkway drive suite 100 hanover, md 21076 phone: 1.866.skyrizi (1.866.759.7494) to join today. Web use this checklist from skyrizi complete to start and stay on track with your prescribed treatment plan. This fax may contain medical information that is privileged and. Once enrolled, you can expect a call from your nurse ambassador within. If approved, we will ship the medication to the patient’s home unless otherwise indicated on the application.

Optumrx form Fill out & sign online DocHub
Web download and fill out the skyrizi complete enrollment and prescription form with your patient. If approved, we will ship the medication to the patient’s home unless otherwise indicated on the application. The call may come from any area code. This fax may contain medical information that is privileged and. 1.866.skyrizi (1.866.759.7494) to join today.
Skyrizi Enrollment Form Enrollment Form
1.866.skyrizi (1.866.759.7494) to join today. Web use this checklist from skyrizi complete to start and stay on track with your prescribed treatment plan. This fax may contain medical information that is privileged and. If approved, we will ship the medication to the patient’s home unless otherwise indicated on the application. After submitting the form via fax, your patient will receive.

Skyrizi (risankizumab) Crohns PSP Form AbbVie Care 2022 EN World OSCAR
North chicago, il 60064 phone: If approved, we will ship the medication to the patient’s home unless otherwise indicated on the application. Web use this checklist from skyrizi complete to start and stay on track with your prescribed treatment plan. Skyrizi is indicated for the treatment of moderate to severe plaque psoriasis in adults who are candidates for systemic therapy.
65J 1833319 COMPLETE Enrollment FORM Gastro Fill Out and Sign
Skyrizi is indicated for the treatment of moderate to severe plaque psoriasis in adults who are candidates for systemic therapy or phototherapy. Web use this checklist from skyrizi complete to start and stay on track with your prescribed treatment plan. Web print and complete the enrollment form on page 4. Provide your consent for eligibility determination by checking the boxes.
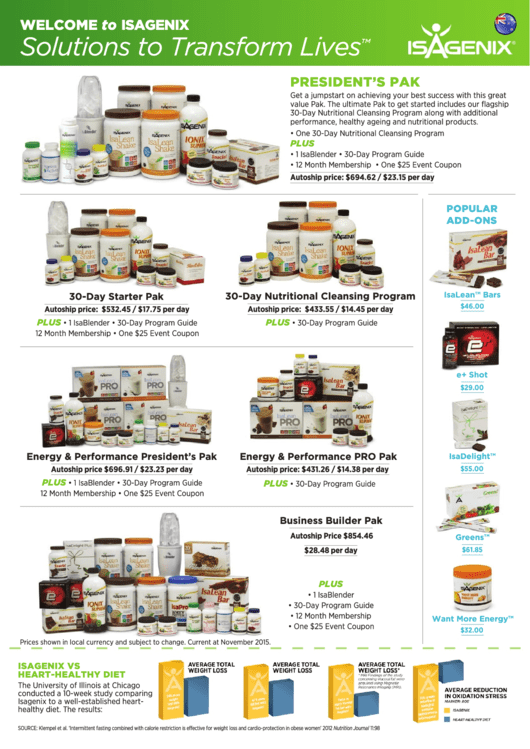
Isagenix Enrollment Form printable pdf download
Web enrolling your patients in skyrizi complete will provide your patients the support to start and stay on track with their prescribed treatment, including the resources below. Help with access & treatment affordability access & savings empower patients nurse ambassadors* insurance support when needed access specialists Skyrizi is indicated for the treatment of active psoriatic arthritis in adults. If approved,.

NICE’s fasttrack catapults Skyrizi into market PMLiVE
Web print and complete the enrollment form on page 4. 1 / / / / Help with access & treatment affordability access & savings empower patients nurse ambassadors* insurance support when needed access specialists You must also provide a separate signature and date for hipaa authorization. 1.866.skyrizi (1.866.759.7494) to join today.

Skyrizi (risankizumab) PSP Form AbbVie Care EN Juno EMR Support Portal
If approved, we will ship the medication to the patient’s home unless otherwise indicated on the application. Once enrolled, you can expect a call from your nurse ambassador within. Provide your consent for eligibility determination by checking the boxes in section 5 and confirm your understanding of the terms of participation by providing your signature and date. Priority partners 7231.

Optumrx New Form Fill Online, Printable, Fillable, Blank pdfFiller
You must also provide a separate signature and date for hipaa authorization. Web enrolling your patients in skyrizi complete will provide your patients the support to start and stay on track with their prescribed treatment, including the resources below. Web use this checklist from skyrizi complete to start and stay on track with your prescribed treatment plan. Once enrolled, you.

Student Enrollment Form California Free Download
Provide your consent for eligibility determination by checking the boxes in section 5 and confirm your understanding of the terms of participation by providing your signature and date. Web print and complete the enrollment form on page 4. Web enrolling your patients in skyrizi complete will provide your patients the support to start and stay on track with their prescribed.
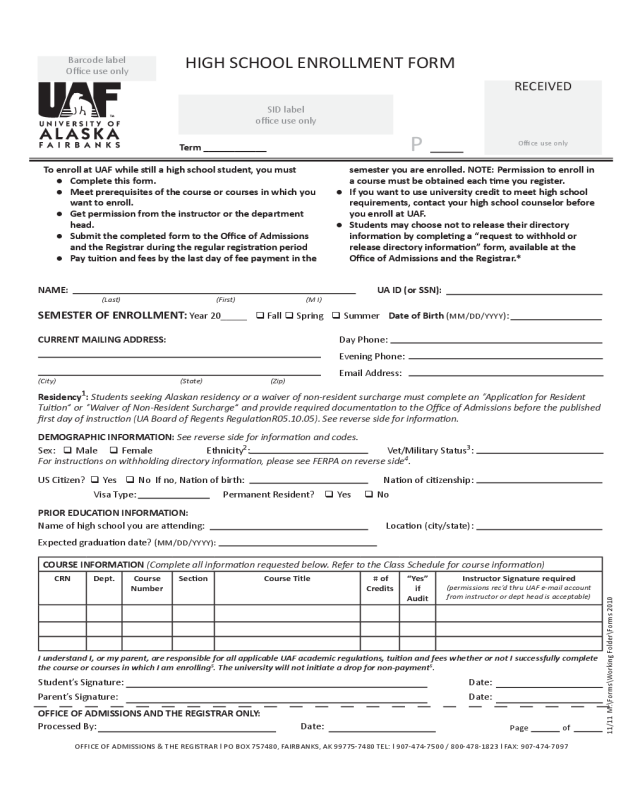
2021 Student Enrollment Form Fillable, Printable PDF & Forms Handypdf
You must also provide a separate signature and date for hipaa authorization. After submitting the form via fax, your patient will receive a call from a nurse ambassador.* you may also complete the pharmacy prescription form and fax it to your patient's specialty pharmacy. 1 / / / / Priority partners 7231 parkway drive suite 100 hanover, md 21076 phone:.
The Call May Come From Any Area Code.
Web print and complete the enrollment form on page 4. Priority partners 7231 parkway drive suite 100 hanover, md 21076 phone: Web download and fill out the skyrizi complete enrollment and prescription form with your patient. Once enrolled, you can expect a call from your nurse ambassador within.
This Fax May Contain Medical Information That Is Privileged And.
1.866.skyrizi (1.866.759.7494) to join today. After submitting the form via fax, your patient will receive a call from a nurse ambassador.* you may also complete the pharmacy prescription form and fax it to your patient's specialty pharmacy. You must also provide a separate signature and date for hipaa authorization. North chicago, il 60064 phone:
Web Use This Checklist From Skyrizi Complete To Start And Stay On Track With Your Prescribed Treatment Plan.
Help with access & treatment affordability access & savings empower patients nurse ambassadors* insurance support when needed access specialists 1 / / / / Skyrizi is indicated for the treatment of moderate to severe plaque psoriasis in adults who are candidates for systemic therapy or phototherapy. If approved, we will ship the medication to the patient’s home unless otherwise indicated on the application.
Skyrizi Is Indicated For The Treatment Of Active Psoriatic Arthritis In Adults.
Provide your consent for eligibility determination by checking the boxes in section 5 and confirm your understanding of the terms of participation by providing your signature and date. Web enrolling your patients in skyrizi complete will provide your patients the support to start and stay on track with their prescribed treatment, including the resources below.