Ocfs Medical Form
Ocfs Medical Form - If the only role is a household member, complete ony the front page. 04/2016) page 3 of 4 is consent of child's parent or guardian for routine medical care on file? Ocfs forms and publications unit. A signature is required on both sides of this form. Web this form may be used to meet the consent requirements for the administration of the following: Web office of children and family services child in care medical statement to be completed by licensed physician, physician assistant or nurse practitioner name of child: Yes no * a copy of the well visit can be attached to this form a signature is required. Request for forms and publications to: Or call the publications hotline: 06/2019) new york state office of children and family services child in care medical statement to be completed by licensed physician, physician assistant or nurse practitioner name of child:
Yes no * a copy of the well visit can be attached to this form a signature is required. 04/2016) page 3 of 4 is consent of child's parent or guardian for routine medical care on file? Ocfs forms and publications unit. / / date of examination: Web office of children and family services child in care medical statement to be completed by licensed physician, physician assistant or nurse practitioner name of child: If the only role is a household member, complete ony the front page. Request for forms and publications to: 7/2005) front new york state office of children and family services medical statement of child in childcare to be completed by licensed physician, physician’s assistant or nurse practitioner name of child: Immunizations required for entry into day care medical exemption Web this form may be used to meet the consent requirements for the administration of the following:
/ / date of examination: If the only role is a household member, complete ony the front page. Request for forms and publications to: Or call the publications hotline: Web office of children and family services child in care medical statement to be completed by licensed physician, physician assistant or nurse practitioner name of child: 06/2019) new york state office of children and family services child in care medical statement to be completed by licensed physician, physician assistant or nurse practitioner name of child: 7/2005) front new york state office of children and family services medical statement of child in childcare to be completed by licensed physician, physician’s assistant or nurse practitioner name of child: Only those staff certified to administer medications to day care children are permitted to do so. Yes no * a copy of the well visit can be attached to this form a signature is required. / / immunizations required for entry into day care

Ocfsmedical Statement of Child in Childcare Diseases And Disorders
/ / date of examination: Yes no * a copy of the well visit can be attached to this form a signature is required. Only those staff certified to administer medications to day care children are permitted to do so. / / immunizations required for entry into day care Ocfs forms and publications unit.
Ocfs Medication Administration Forms Daycare Fill Online, Printable
Or call the publications hotline: Ocfs forms and publications unit. 7/2005) front new york state office of children and family services medical statement of child in childcare to be completed by licensed physician, physician’s assistant or nurse practitioner name of child: Request for forms and publications to: 04/2016) page 3 of 4 is consent of child's parent or guardian for.
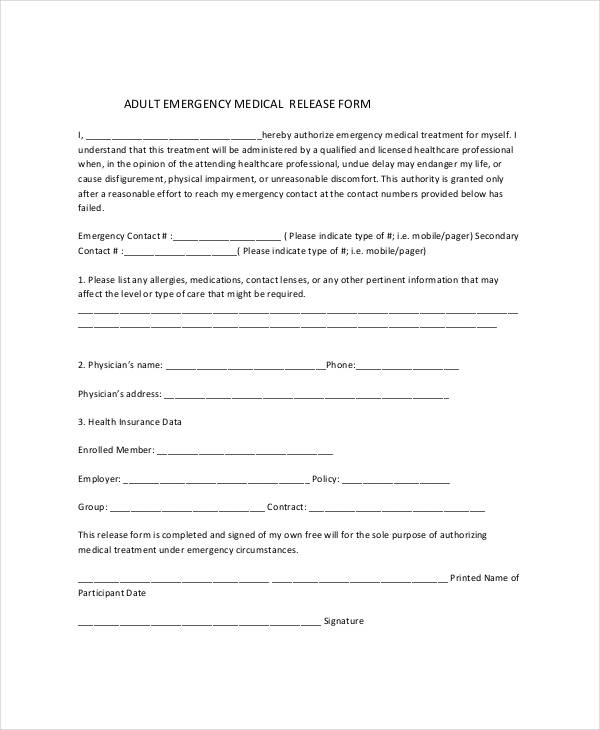
FREE 27+ Sample Medical Release Forms in PDF Excel MS Word
Web this form may be used to meet the consent requirements for the administration of the following: If the only role is a household member, complete ony the front page. A signature is required on both sides of this form. Web office of children and family services child in care medical statement to be completed by licensed physician, physician assistant.

NY OCFSLDSS0792 20052021 Fill and Sign Printable Template Online
If the only role is a household member, complete ony the front page. Request for forms and publications to: Web office of children and family services child in care medical statement to be completed by licensed physician, physician assistant or nurse practitioner name of child: Ocfs forms and publications unit. Web this form may be used to meet the consent.
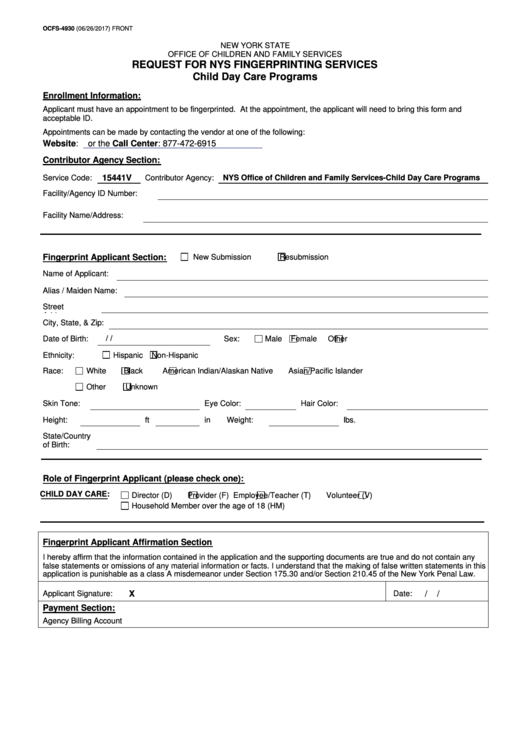
Form Ocfs4930 Request For Nys Fingerprinting Services Nys Office
Web office of children and family services child in care medical statement to be completed by licensed physician, physician assistant or nurse practitioner name of child: Yes no * a copy of the well visit can be attached to this form a signature is required. 06/2019) new york state office of children and family services child in care medical statement.
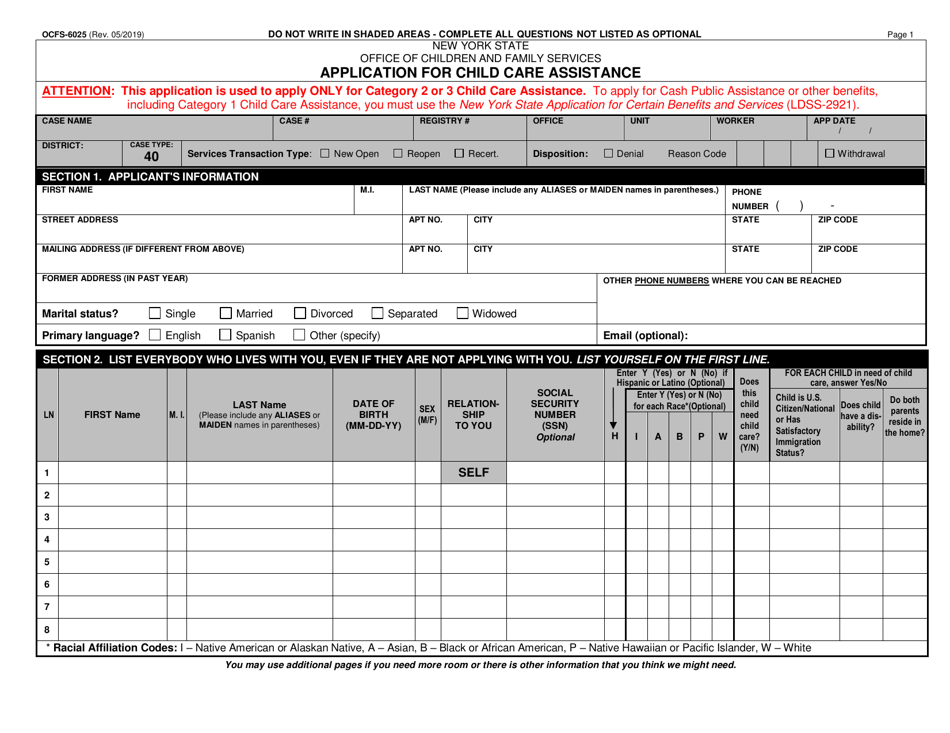
Form OCFS6025 Download Printable PDF or Fill Online Application for
04/2016) page 3 of 4 is consent of child's parent or guardian for routine medical care on file? Web office of children and family services child in care medical statement to be completed by licensed physician, physician assistant or nurse practitioner name of child: Or call the publications hotline: A signature is required on both sides of this form. 7/2005).
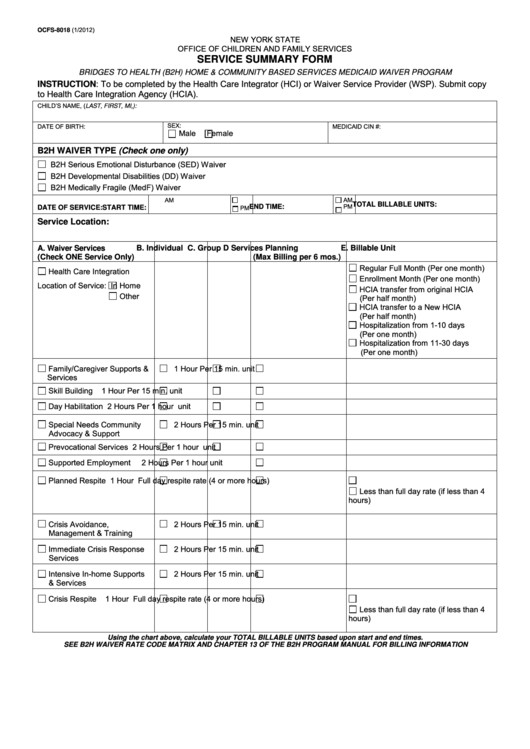
Fillable Service Summary Form Ocfs New York State printable pdf
06/2019) new york state office of children and family services child in care medical statement to be completed by licensed physician, physician assistant or nurse practitioner name of child: Yes no * a copy of the well visit can be attached to this form a signature is required. Immunizations required for entry into day care medical exemption If the only.
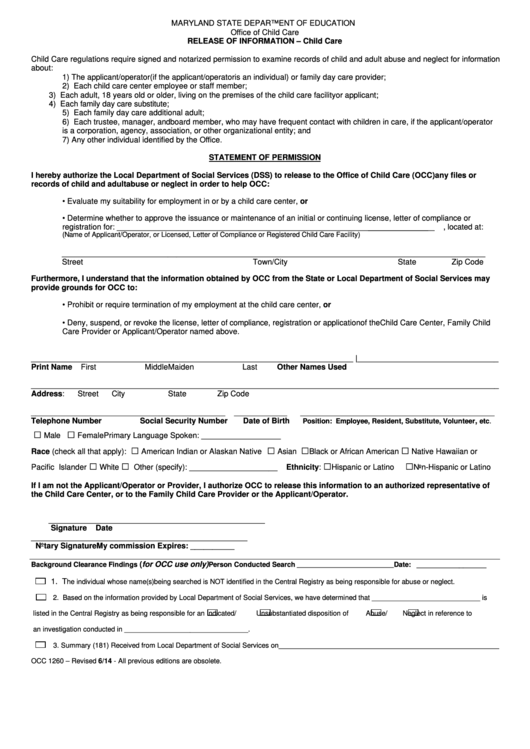
Form Occ 1260 Release Of Information Child Care printable pdf download
Immunizations required for entry into day care medical exemption Web office of children and family services child in care medical statement to be completed by licensed physician, physician assistant or nurse practitioner name of child: If the only role is a household member, complete ony the front page. / / date of examination: A signature is required on both sides.
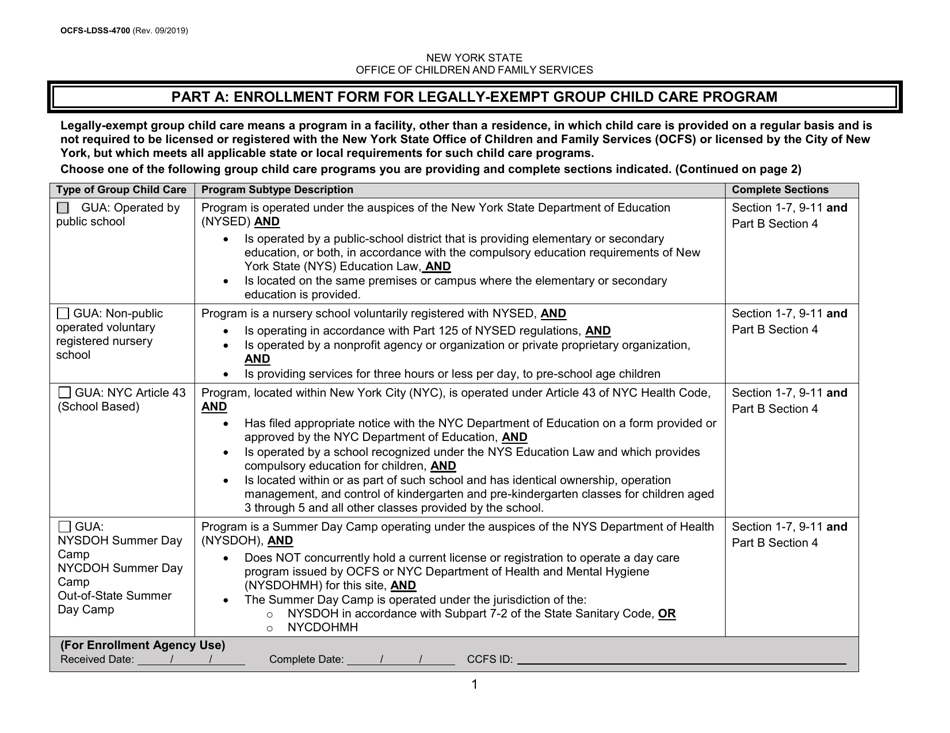
Form OCFSLDSS4700 Part A Download Printable PDF or Fill Online
Ocfs forms and publications unit. A signature is required on both sides of this form. 04/2016) page 3 of 4 is consent of child's parent or guardian for routine medical care on file? Web office of children and family services child in care medical statement to be completed by licensed physician, physician assistant or nurse practitioner name of child: Only.

Medical Report Form Lobo Black in 2020 Report template, Pamphlet
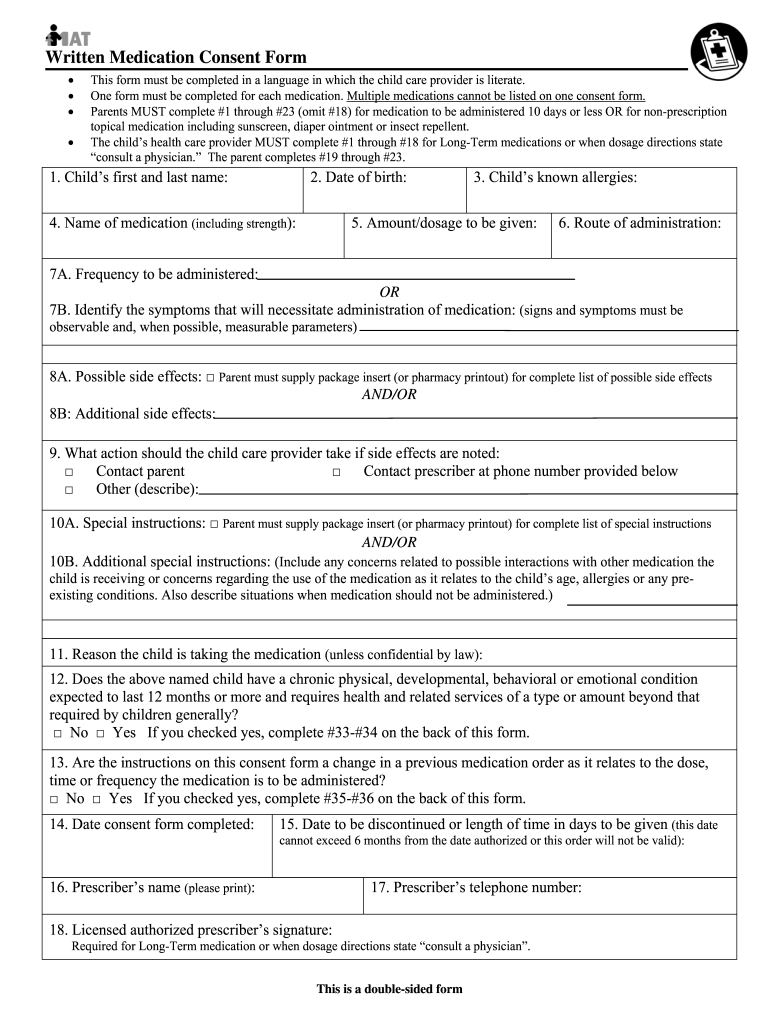
Web this form may be used to meet the consent requirements for the administration of the following: / / immunizations required for entry into day care Only those staff certified to administer medications to day care children are permitted to do so. Web office of children and family services child in care medical statement to be completed by licensed physician,.
Web This Form May Be Used To Meet The Consent Requirements For The Administration Of The Following:
Ocfs forms and publications unit. Web office of children and family services child in care medical statement to be completed by licensed physician, physician assistant or nurse practitioner name of child: A signature is required on both sides of this form. Request for forms and publications to:
04/2016) Page 3 Of 4 Is Consent Of Child's Parent Or Guardian For Routine Medical Care On File?
If the only role is a household member, complete ony the front page. / / date of examination: 7/2005) front new york state office of children and family services medical statement of child in childcare to be completed by licensed physician, physician’s assistant or nurse practitioner name of child: Or call the publications hotline:
/ / Immunizations Required For Entry Into Day Care
Only those staff certified to administer medications to day care children are permitted to do so. Immunizations required for entry into day care medical exemption Yes no * a copy of the well visit can be attached to this form a signature is required. 06/2019) new york state office of children and family services child in care medical statement to be completed by licensed physician, physician assistant or nurse practitioner name of child: