Hcfa Form Pdf
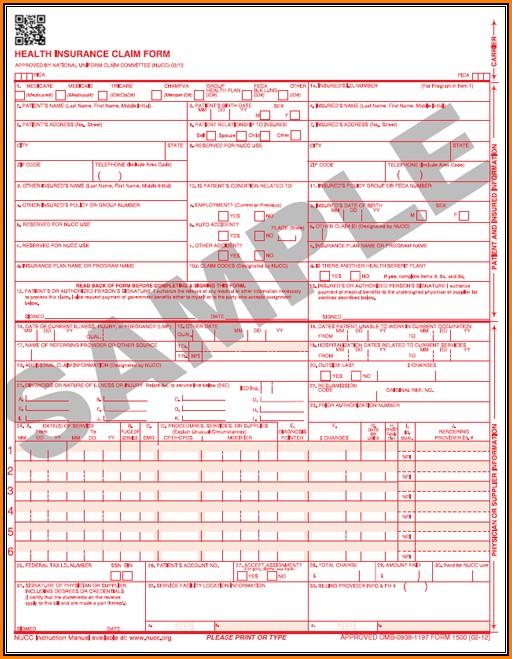
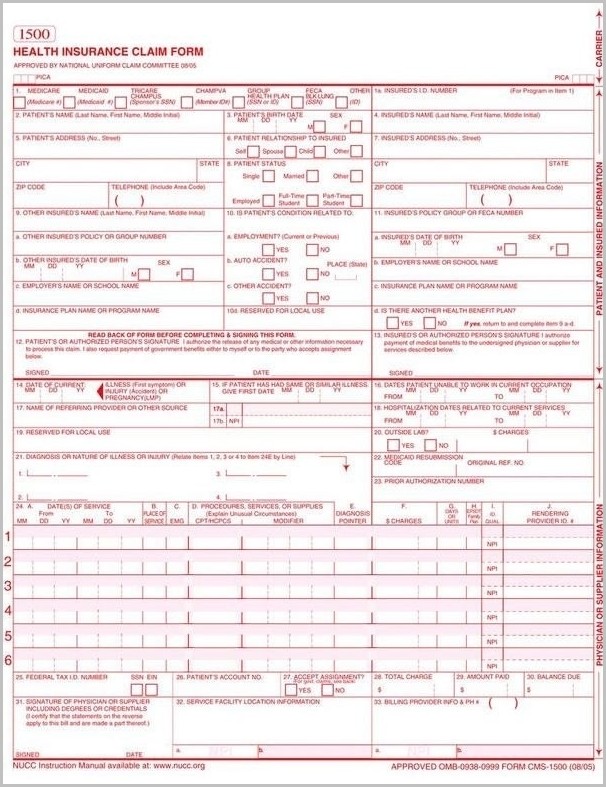
Hcfa Form Pdf - Web compensation act (feca), the black lung benefits act (blba), and the energy employees occupational illness compensation program act. Read the instructions and tips below first. Indicate the date to the sample using the date tool. Payer type of the destination. Will be denied or returned. Download or email cms 1500 & more fillable forms, register and subscribe now! Web cms 1500 form telephone number. Web cms 1500 dynamic list information. Web fillable hcfa 1500 claim form. Web reset form print form 1500 health insurance claim form approved by national uniform claim committee 08/05.
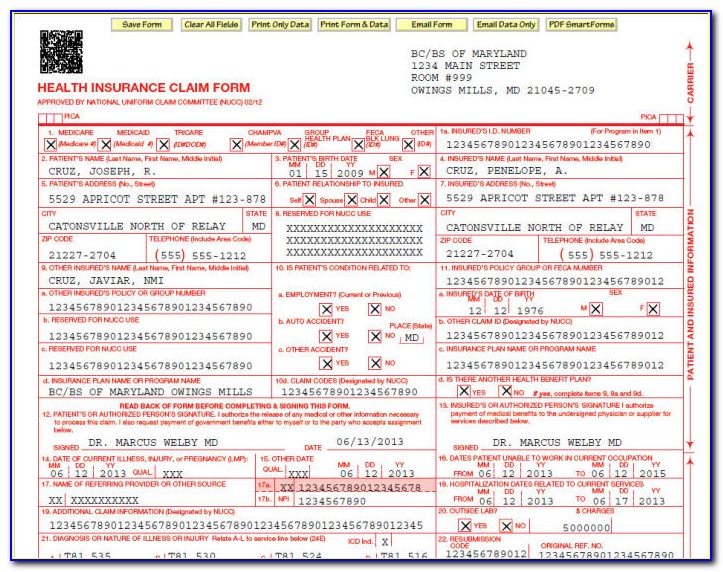
Web cms 1500 dynamic list information. Check the appropriate box for the patient’s relationship to the. Sign online button or tick the preview image of the blank. Ensure the information you fill in hcfa 1500 is updated and accurate. Web complete blank form of hcfa online with us legal forms. Save or instantly send your ready documents. • the 1500 claim form is developed and maintained by the nucc. Item 6 patient’s relationship to insured if medicare is primary, leave blank. Web fill in each fillable field. Easily fill out pdf blank, edit, and sign them.
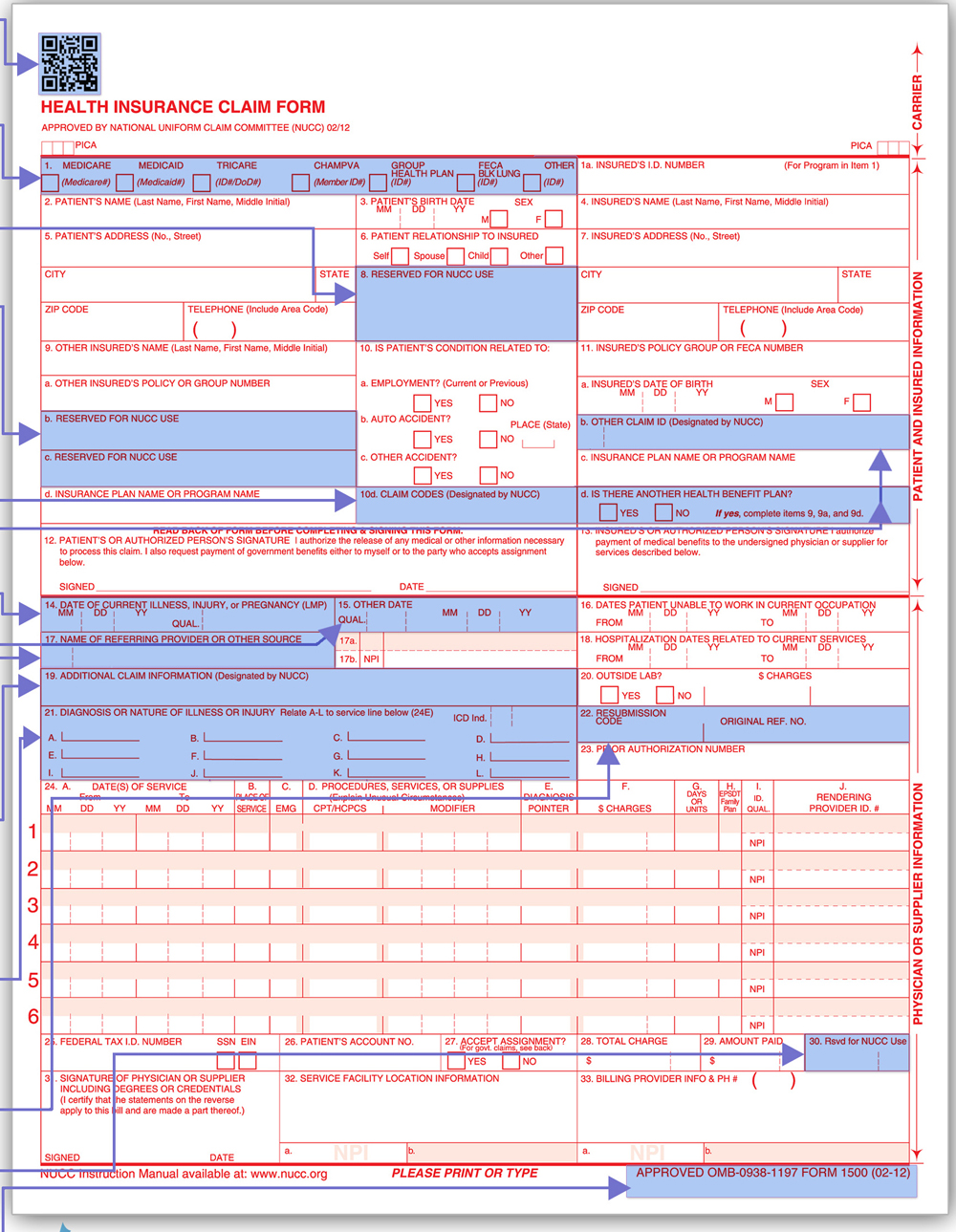
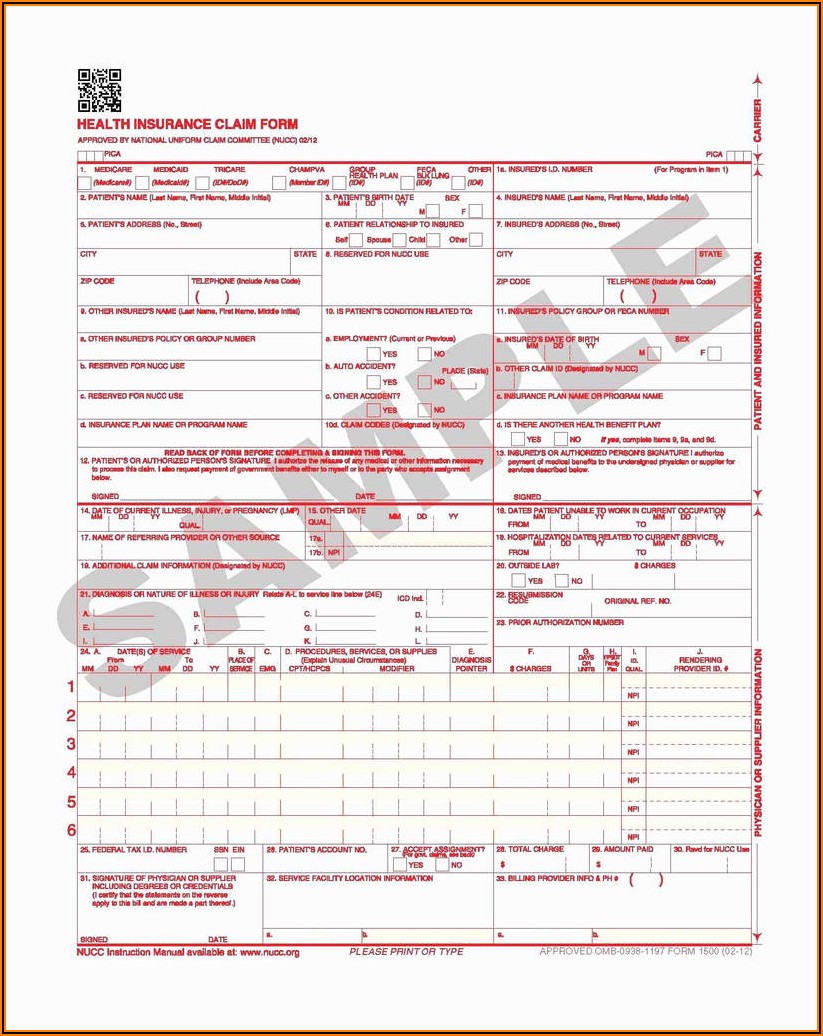
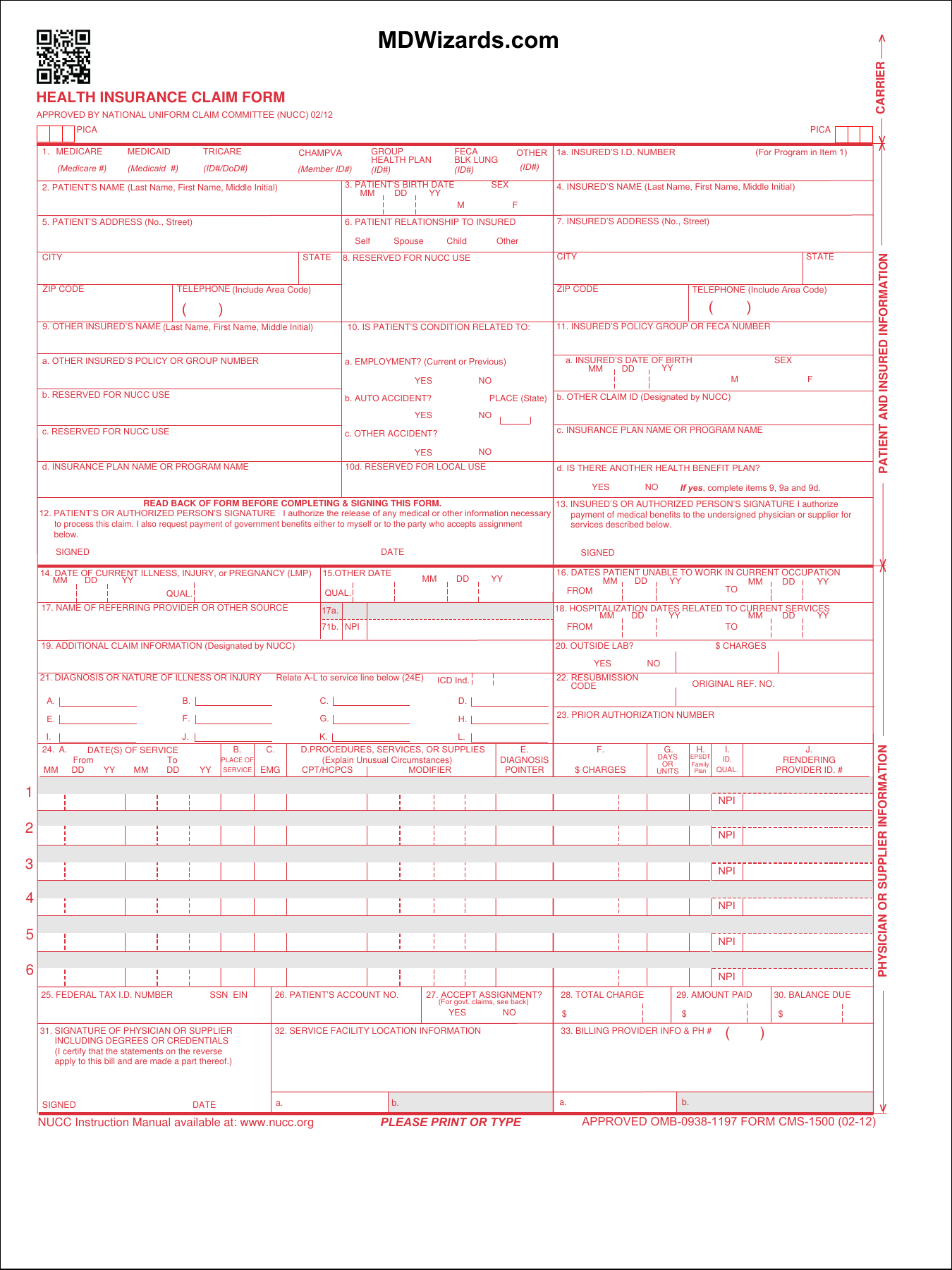
Web how to edit the hcfa 1500 form conviniently online. Print only on official cms 1500. Start on editing, signing and sharing your hcfa 1500 form online under the guide of these easy steps: Read the instructions and tips below first. Item 6 patient’s relationship to insured if medicare is primary, leave blank. Will be denied or returned. Insured’s name (last name, first name, middle initial) 7. Download free cms 1500 claim form fillable template. Web health insurance claim form 1. Table 1 explains each of the boxes in the hcfa form.
Form Hcfa 1500 Form Resume Examples 4x2v1DQV5l
Sign online button or tick the preview image of the blank. • the 1500 claim form is developed and maintained by the nucc. Check the appropriate box for the patient’s relationship to the. Web cms 1500 form telephone number. Web how to complete the cfa claim form online:
Hcfa 1500 Form Sample Form Resume Examples
Web fillable hcfa 1500 claim form. Push the get form or. Web cms 1500 dynamic list information. Start on editing, signing and sharing your hcfa 1500 form online under the guide of these easy steps: Will be denied or returned.
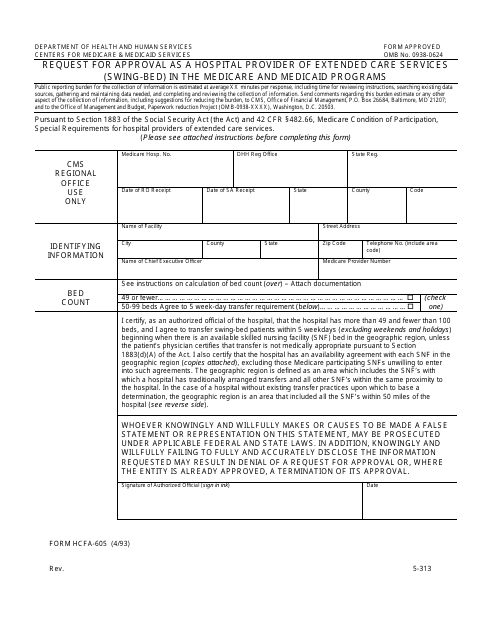
Form HCFA605 Download Printable PDF or Fill Online Request for
Any one who misrepresents or. Download free cms 1500 claim form fillable template. Indicate the date to the sample using the date tool. 2.33 out of 5) download the fillable hcfa 1500 claim form that is both a fillable and/or printable medical claim form that. Web cms 1500 form telephone number.

HealthCare Mafia
Web cms 1500 form telephone number. Web complete blank form of hcfa online with us legal forms. Save or instantly send your ready documents. Click on the sign button and make a. Easily fill out pdf blank, edit, and sign them.
HCFA Forms 1 Part Continuous REVISED
• the 1500 claim form is developed and maintained by the nucc. Number (for program in item 1) 4. Sign online button or tick the preview image of the blank. Web fillable hcfa 1500 claim form. Insured’s name (last name, first name, middle initial) 7.

Hcfa 1500 Form Pdf Form Resume Examples 46V3RQvK7b
Web health insurance claim form 1. Will be denied or returned. Click on the sign button and make a. Ensure the information you fill in hcfa 1500 is updated and accurate. Medicare medicaid tricare champva other read back of form before completing & signing this form.

Hcfa 1500 Form Pdf Fillable Form Resume Examples
Medicare medicaid tricare champva other read back of form before completing & signing this form. Web compensation act (feca), the black lung benefits act (blba), and the energy employees occupational illness compensation program act. Web how to edit the hcfa 1500 form conviniently online. Web cms 1500 dynamic list information. Will be denied or returned.
Hcfa 1500 Form Download Pdf Form Resume Examples xz20pPEZ2q
Web how to complete the cfa claim form online: Web how to edit the hcfa 1500 form conviniently online. Web no part b medicare benefits may be paid unless this form is received as required by existing law and regulations (42 cfr 424.32). Medicare medicaid tricare champva other read back of form before completing & signing this form. Web cms.
Download Fillable HCFA 1500 Claim Form PDF RTF Word
Insured’s name (last name, first name, middle initial) 7. Web fillable hcfa 1500 claim form. Start on editing, signing and sharing your hcfa 1500 form online under the guide of these easy steps: Any one who misrepresents or. Indicate the date to the sample using the date tool.
Cms Hcfa 1500 Form Pdf Form Resume Examples EpDLyEE5xR
Web understanding your hcfa 1500 claim form making sense of medicare paperwork, including the hcfa 1500 claim form, can be difficult. Will be denied or returned. In addition, cms will use the generic or chemical name if there are no other similar chemical products on the market. Read the instructions and tips below first. Check the appropriate box for the.
Medicare Medicaid Tricare Champva Other Read Back Of Form Before Completing & Signing This Form.
Table 1 explains each of the boxes in the hcfa form. Read the instructions and tips below first. Push the get form or. Download free cms 1500 claim form fillable template.
Easily Fill Out Pdf Blank, Edit, And Sign Them.
Print only on official cms 1500. Web how to complete the cfa claim form online: Item 6 patient’s relationship to insured if medicare is primary, leave blank. Web complete blank form of hcfa online with us legal forms.
Ensure The Information You Fill In Hcfa 1500 Is Updated And Accurate.
Web fillable hcfa 1500 claim form. Number (for program in item 1) 4. Sign online button or tick the preview image of the blank. Web fill in each fillable field.
• The 1500 Claim Form Is Developed And Maintained By The Nucc.
Web understanding your hcfa 1500 claim form making sense of medicare paperwork, including the hcfa 1500 claim form, can be difficult. Web compensation act (feca), the black lung benefits act (blba), and the energy employees occupational illness compensation program act. Insured’s name (last name, first name, middle initial) 7. Save or instantly send your ready documents.