Free Fillable Ub 04 Form Pdf
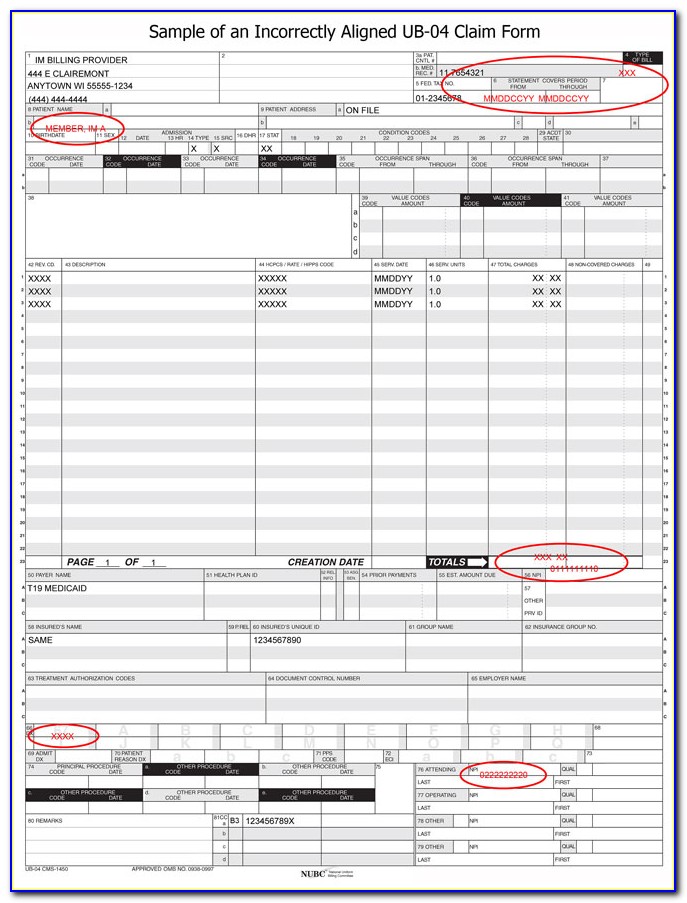
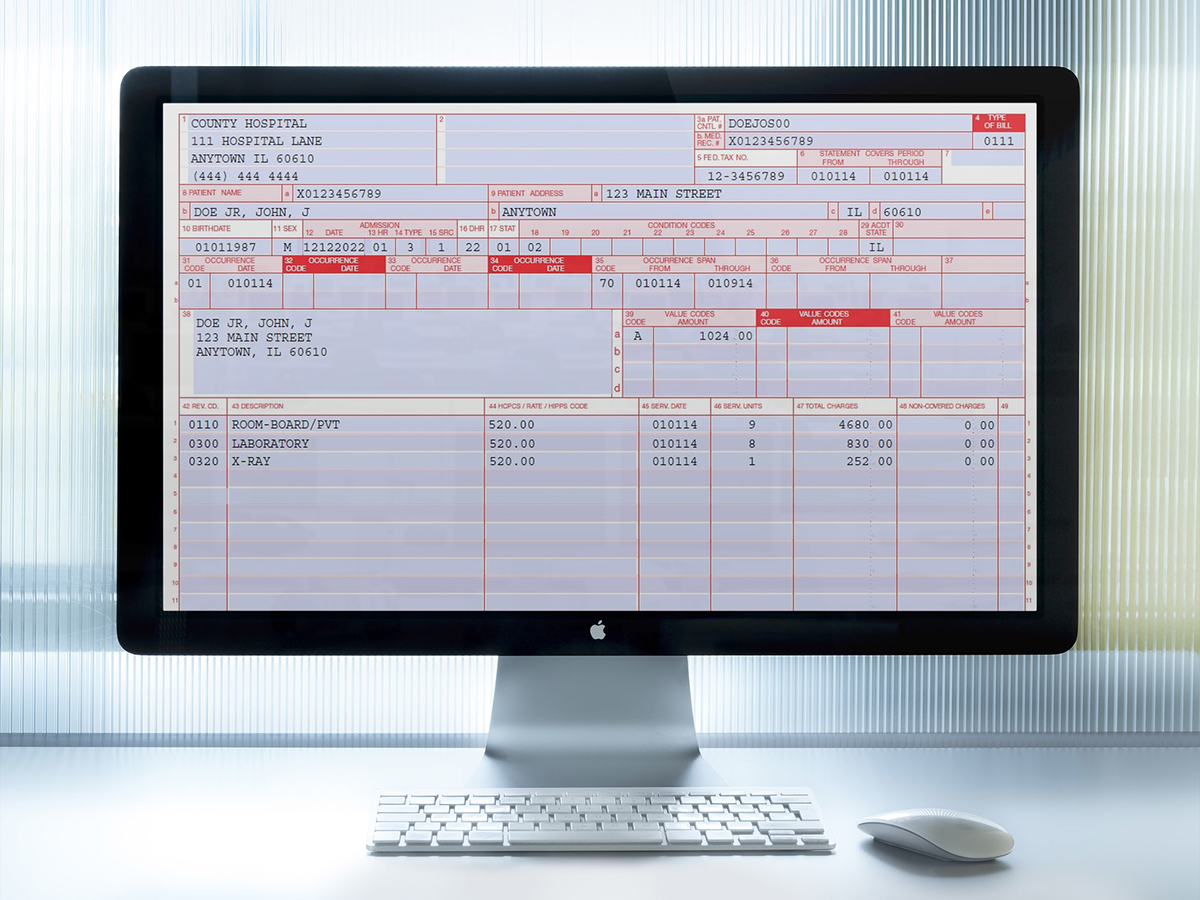
Free Fillable Ub 04 Form Pdf - Next, identify and provide the specific details about the healthcare facility where the services were rendered. Once completed you can sign your fillable form or send for. Web how to fill out ub04 form. The following ub04 guide is for educational purposes and does not ensure payment. The submitter of this form underst ands that misrepresent ation or f alsification of essential information as requested by this form, may serve as the basis for civil monetarty penalties and assessments and may upon conviction include fines and/or imprisonment under federal and/or state law(s). Use fill to complete blank online entyvio pdf forms for free. Web fill online, printable, fillable, blank hospital outpatient sample ub 04 claim form (entyvio) form. Bluecare plus follows the center for medicare & medicaid services (cms) guidelines for filing the national provider identifier (npi) number. Form locator description ub 04 field 1 billing provider name, address, This includes their name, address, date of birth, and insurance information.
Web fill online, printable, fillable, blank hospital outpatient sample ub 04 claim form (entyvio) form. To fill out a ub04 form, start by entering the patient's information in the designated fields. Use fill to complete blank online entyvio pdf forms for free. Save the file as a pdf document to your computer. Once completed you can sign your fillable form or send for. The submitter of this form underst ands that misrepresent ation or f alsification of essential information as requested by this form, may serve as the basis for civil monetarty penalties and assessments and may upon conviction include fines and/or imprisonment under federal and/or state law(s). The following ub04 guide is for educational purposes and does not ensure payment. Then you can do either of the following: This includes their name, address, date of birth, and insurance information. Print the file so that you have a hardcopy.
Use fill to complete blank online entyvio pdf forms for free. Form locator description ub 04 field 1 billing provider name, address, The submitter of this form underst ands that misrepresent ation or f alsification of essential information as requested by this form, may serve as the basis for civil monetarty penalties and assessments and may upon conviction include fines and/or imprisonment under federal and/or state law(s). Web how to fill out ub04 form. Save the file as a pdf document to your computer. Print the file so that you have a hardcopy. This includes their name, address, date of birth, and insurance information. To fill out a ub04 form, start by entering the patient's information in the designated fields. The following ub04 guide is for educational purposes and does not ensure payment. Web fill online, printable, fillable, blank hospital outpatient sample ub 04 claim form (entyvio) form.
W 9 Form Fillable Free Form Resume Examples 7mk9Mo4kGY
Use fill to complete blank online entyvio pdf forms for free. To fill out a ub04 form, start by entering the patient's information in the designated fields. This includes their name, address, date of birth, and insurance information. The submitter of this form underst ands that misrepresent ation or f alsification of essential information as requested by this form, may.

Free Fillable Ub 04 Form Pdf Form Resume Examples o85pJVbkZJ
Once completed you can sign your fillable form or send for. Use fill to complete blank online entyvio pdf forms for free. The submitter of this form underst ands that misrepresent ation or f alsification of essential information as requested by this form, may serve as the basis for civil monetarty penalties and assessments and may upon conviction include fines.
Creditor Claim Form Form Resume Examples rykgyKj5wn
Next, identify and provide the specific details about the healthcare facility where the services were rendered. Inpatient hospital facilities, such as medical/surgical intensive care, burn care, coronary care and ancillary charges (such as labor and delivery, anesthesiology and central services and supplies) This includes their name, address, date of birth, and insurance information. Bluecare plus follows the center for medicare.
Free W 9 Form Fillable Form Resume Examples bX5aMeX5wW
Bluecare plus follows the center for medicare & medicaid services (cms) guidelines for filing the national provider identifier (npi) number. Web fill online, printable, fillable, blank hospital outpatient sample ub 04 claim form (entyvio) form. Use fill to complete blank online entyvio pdf forms for free. Next, identify and provide the specific details about the healthcare facility where the services.
Free Fillable And Printable Ub 04 Claim Form Printable Templates Gambaran
Once completed you can sign your fillable form or send for. To fill out a ub04 form, start by entering the patient's information in the designated fields. Bluecare plus follows the center for medicare & medicaid services (cms) guidelines for filing the national provider identifier (npi) number. This includes their name, address, date of birth, and insurance information. Form locator.
Ub04 Form Fill Online, Printable, Fillable, Blank pdfFiller
Once completed you can sign your fillable form or send for. Web how to fill out ub04 form. Next, identify and provide the specific details about the healthcare facility where the services were rendered. Then you can do either of the following: Use fill to complete blank online entyvio pdf forms for free.

Ub 04 Claim Form Fill Online, Printable, Fillable, Blank pdfFiller
This includes their name, address, date of birth, and insurance information. Web fill online, printable, fillable, blank hospital outpatient sample ub 04 claim form (entyvio) form. Save the file as a pdf document to your computer. Then you can do either of the following: The submitter of this form underst ands that misrepresent ation or f alsification of essential information.
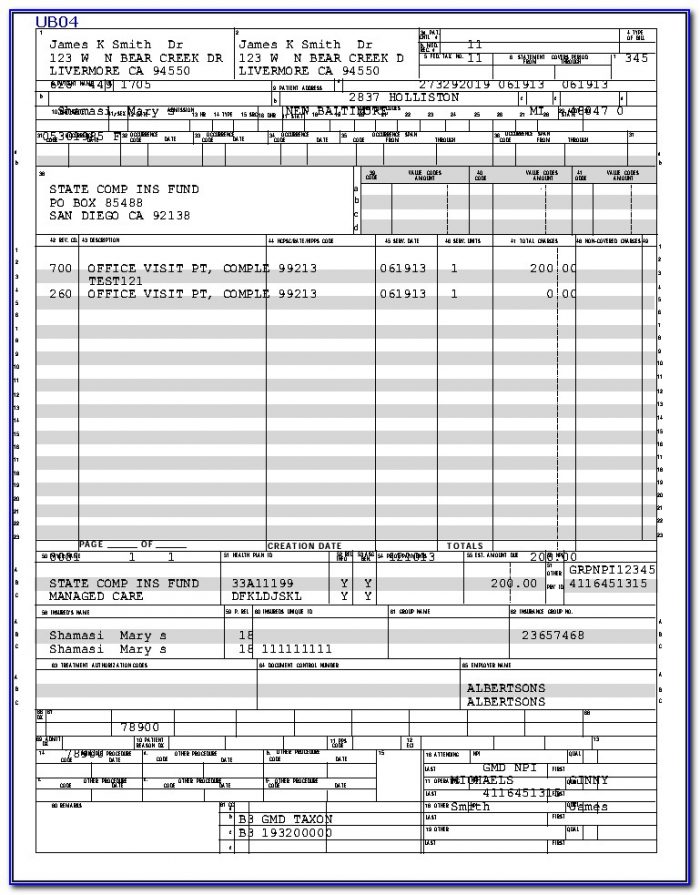
UB04 Uniform Bill Fillable PDF CMS 1450 Fiachra Forms Charting Solutions
Web fill online, printable, fillable, blank hospital outpatient sample ub 04 claim form (entyvio) form. The submitter of this form underst ands that misrepresent ation or f alsification of essential information as requested by this form, may serve as the basis for civil monetarty penalties and assessments and may upon conviction include fines and/or imprisonment under federal and/or state law(s)..
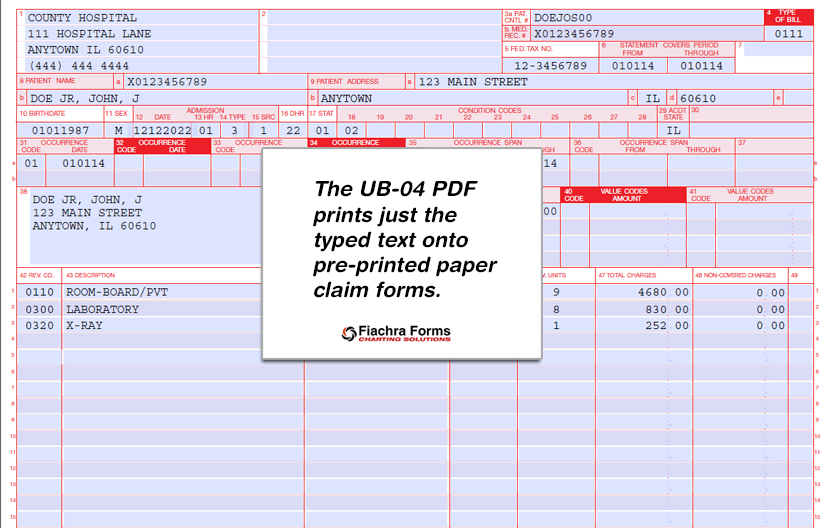
UB 04 PDF Template Fill & Print Health Insurance Claim Form Fiachra
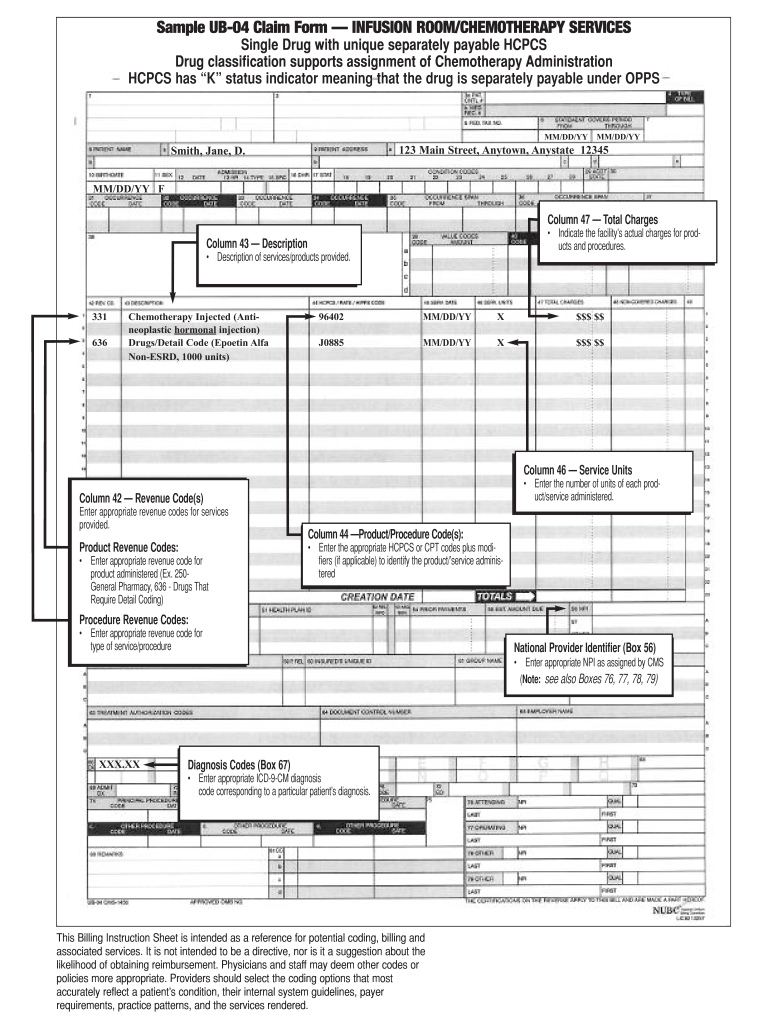
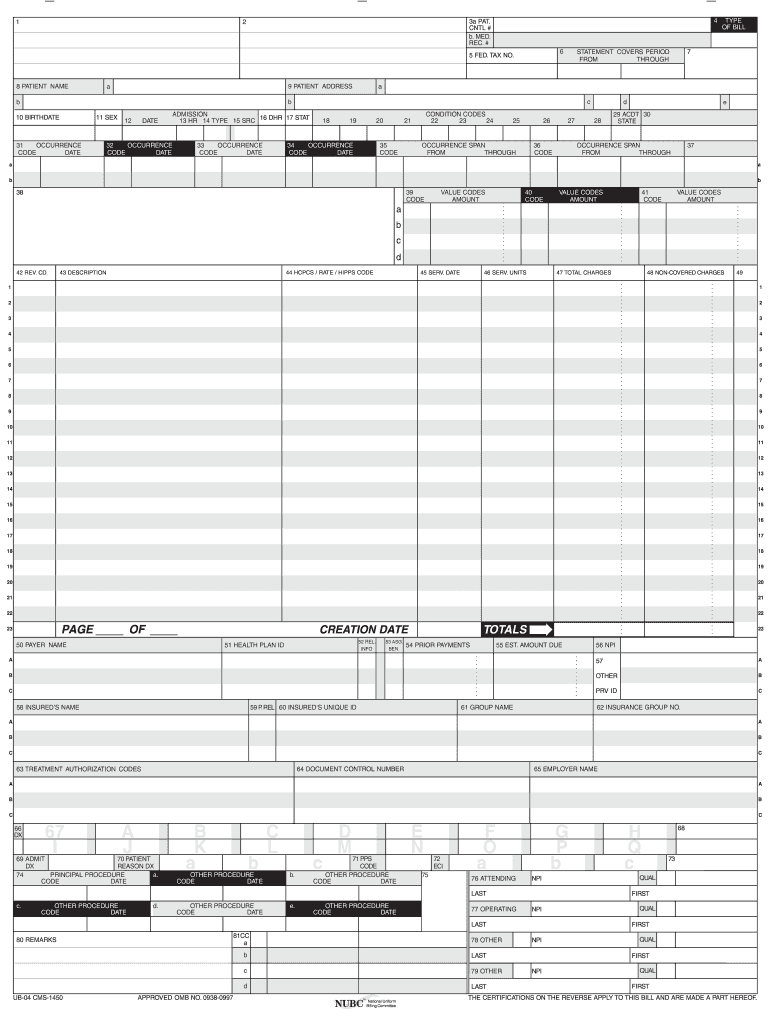
Web fill online, printable, fillable, blank hospital outpatient sample ub 04 claim form (entyvio) form. Save the file as a pdf document to your computer. The following ub04 guide is for educational purposes and does not ensure payment. Form locator description ub 04 field 1 billing provider name, address, Print the file so that you have a hardcopy.
Printable Ub 04 Claim Form Master of Documents
Web how to fill out ub04 form. Form locator description ub 04 field 1 billing provider name, address, Print the file so that you have a hardcopy. Web fill online, printable, fillable, blank hospital outpatient sample ub 04 claim form (entyvio) form. Once completed you can sign your fillable form or send for.
Bluecare Plus Follows The Center For Medicare & Medicaid Services (Cms) Guidelines For Filing The National Provider Identifier (Npi) Number.
Print the file so that you have a hardcopy. Web fill online, printable, fillable, blank hospital outpatient sample ub 04 claim form (entyvio) form. The following ub04 guide is for educational purposes and does not ensure payment. Use fill to complete blank online entyvio pdf forms for free.
Form Locator Description Ub 04 Field 1 Billing Provider Name, Address,
To fill out a ub04 form, start by entering the patient's information in the designated fields. Then you can do either of the following: The submitter of this form underst ands that misrepresent ation or f alsification of essential information as requested by this form, may serve as the basis for civil monetarty penalties and assessments and may upon conviction include fines and/or imprisonment under federal and/or state law(s). Inpatient hospital facilities, such as medical/surgical intensive care, burn care, coronary care and ancillary charges (such as labor and delivery, anesthesiology and central services and supplies)
This Includes Their Name, Address, Date Of Birth, And Insurance Information.
Once completed you can sign your fillable form or send for. Next, identify and provide the specific details about the healthcare facility where the services were rendered. Save the file as a pdf document to your computer. Web how to fill out ub04 form.