Db 450 Form
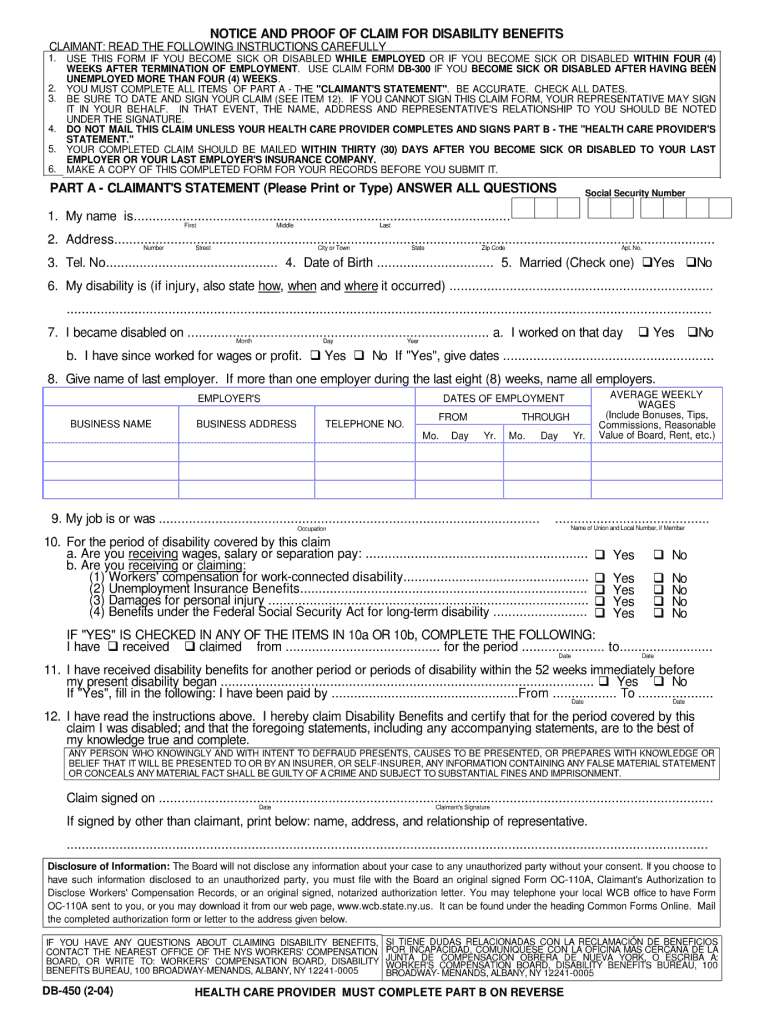
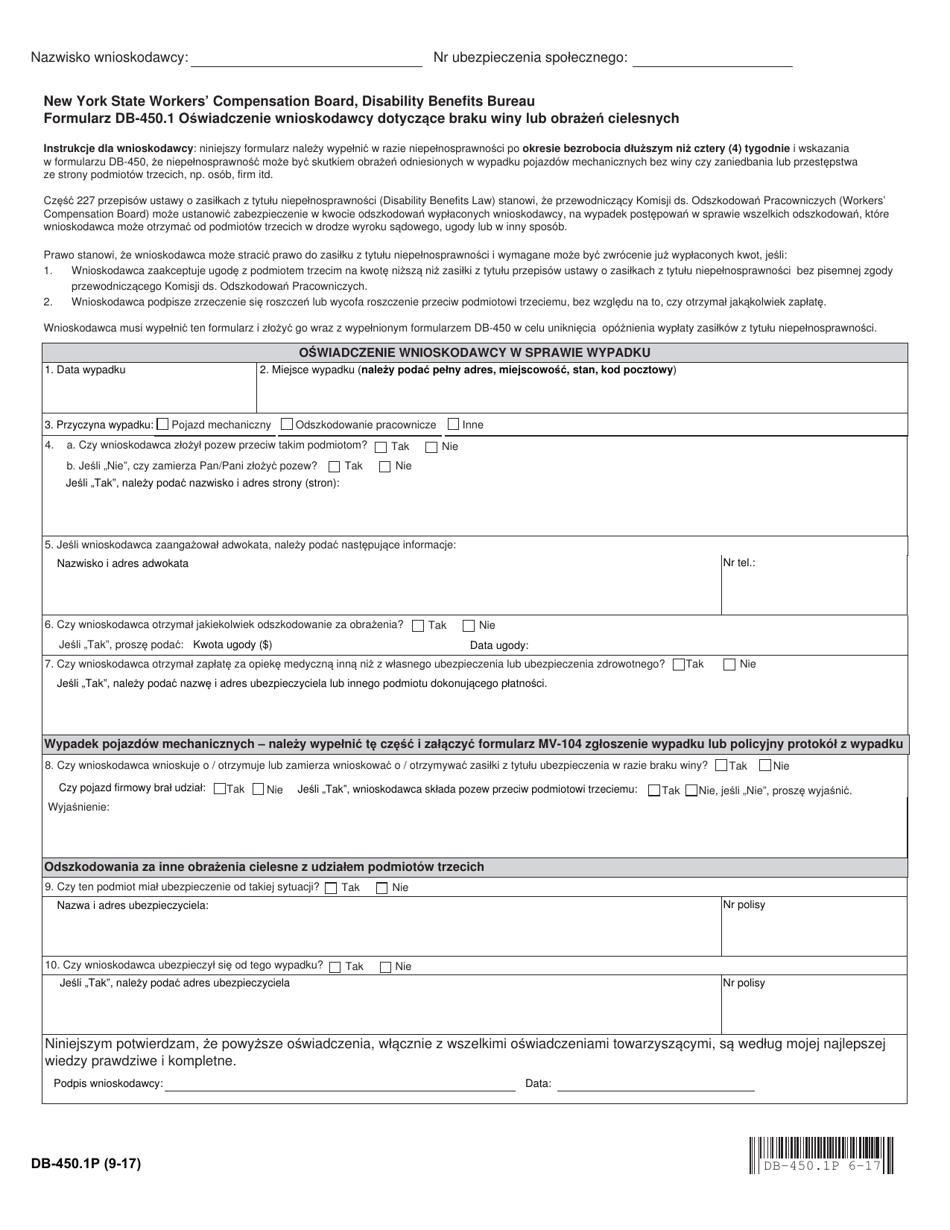
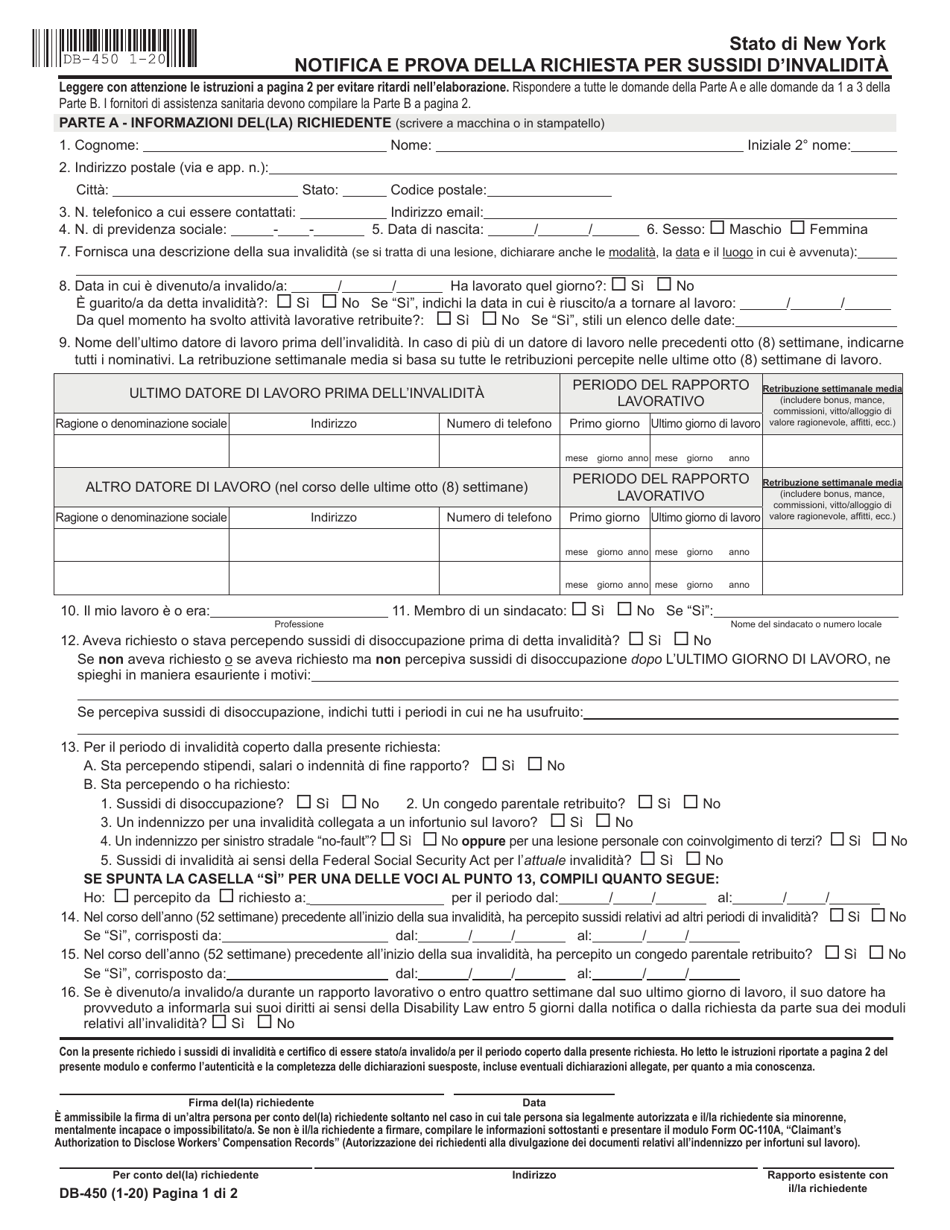
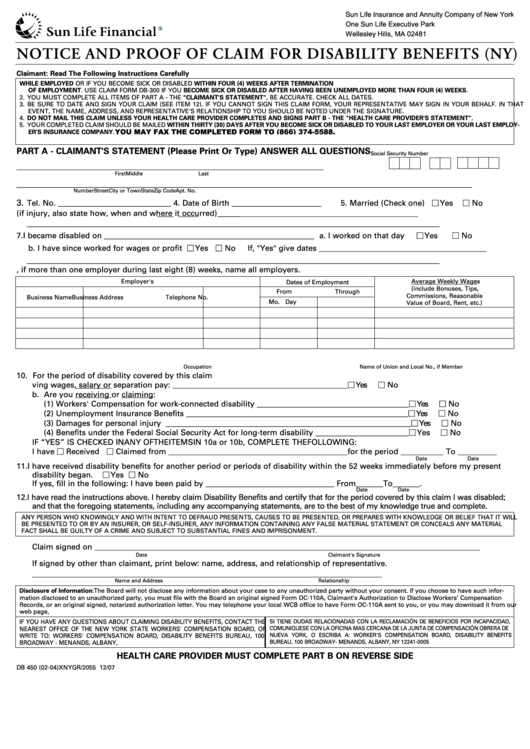
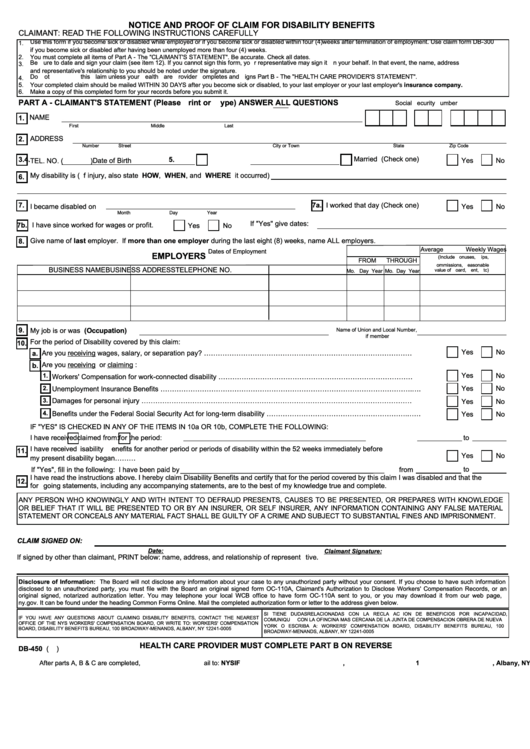
Db 450 Form - Web any employee receiving or entitled to receive social security retirement benefits may submit this form at any time to waive any and all benefits under the disability and paid family leave benefits law: The health care provider's statement must be filled in completely. Mailing address (street & apt. Complete this paperwork if you were working no less than four weeks before the start date of your medical event to apply for benefit payments. For the period of disability covered by this claim: Use this form only when the claimant becomes sick or disabled while employed or becomes sick or disabled within four (4) weeks after termination of employment. Are you receiving or claiming: Are you receiving wages, salary or separation pay? Unemployed for more than four (4) weeks. Pfl 1 & 2 forms
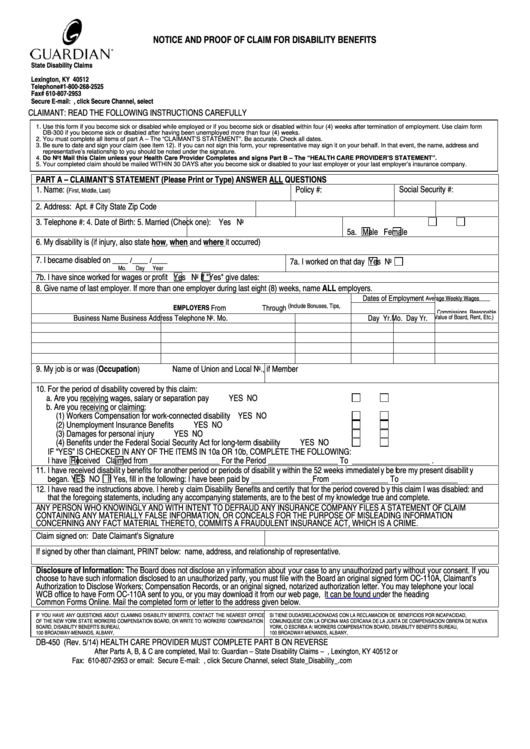
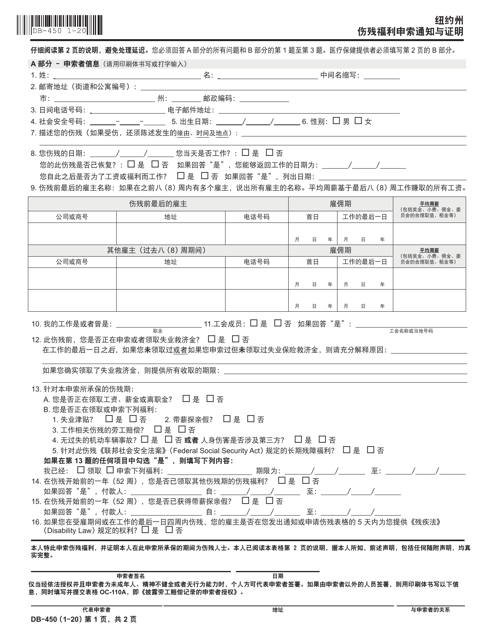
The health care provider's statement must be filled in completely. Web any employee receiving or entitled to receive social security retirement benefits may submit this form at any time to waive any and all benefits under the disability and paid family leave benefits law: Use this form only when the claimant becomes sick or disabled while employed or becomes sick or disabled within four (4) weeks after termination of employment. For the period of disability covered by this claim: Mailing address (street & apt. The attending health care provider shall complete and return to the claimant within seven (7) days of receipt of this form. Are you receiving or claiming: Complete this form if you became disabled after having been. Notice and proof of claim for disability benefits: For approved claims, disability benefits begin on the eighth day of disability.
For approved claims, disability benefits begin on the eighth day of disability. Are you receiving or claiming: Complete this paperwork if you were working no less than four weeks before the start date of your medical event to apply for benefit payments. Notice and proof of claim for disability benefits: Complete this form if you became disabled after having been. Web any employee receiving or entitled to receive social security retirement benefits may submit this form at any time to waive any and all benefits under the disability and paid family leave benefits law: For the period of disability covered by this claim: Are you receiving wages, salary or separation pay? Pfl 1 & 2 forms The health care provider's statement must be filled in completely.
Form Claim Disability Fill Out and Sign Printable PDF Template signNow
Mailing address (street & apt. Are you receiving or claiming: Unemployed for more than four (4) weeks. Notice and proof of claim for disability benefits: Complete this paperwork if you were working no less than four weeks before the start date of your medical event to apply for benefit payments.
Form DB450.1P Download Printable PDF or Fill Online Claimant's
Unemployed for more than four (4) weeks. For the period of disability covered by this claim: Complete this paperwork if you were working no less than four weeks before the start date of your medical event to apply for benefit payments. The attending health care provider shall complete and return to the claimant within seven (7) days of receipt of.
Form DB450I Download Fillable PDF or Fill Online Notice and Proof of
Pfl 1 & 2 forms Web any employee receiving or entitled to receive social security retirement benefits may submit this form at any time to waive any and all benefits under the disability and paid family leave benefits law: Are you receiving wages, salary or separation pay? Notice and proof of claim for disability benefits: The health care provider's statement.
17 Nys Wcb Forms And Templates free to download in PDF
The health care provider's statement must be filled in completely. Notice and proof of claim for disability benefits: The attending health care provider shall complete and return to the claimant within seven (7) days of receipt of this form. Pfl 1 & 2 forms Unemployed for more than four (4) weeks.
New York Notice and Proof of Claim for Disability Benefits for Workers
The health care provider's statement must be filled in completely. The attending health care provider shall complete and return to the claimant within seven (7) days of receipt of this form. Pfl 1 & 2 forms For approved claims, disability benefits begin on the eighth day of disability. Complete this form if you became disabled after having been.
Db450 Form Notice And Proof Of Claim For Disability Benefits (ny
For the period of disability covered by this claim: Are you receiving or claiming: For approved claims, disability benefits begin on the eighth day of disability. Are you receiving wages, salary or separation pay? Mailing address (street & apt.
Db450 Form Notice And Proof Of Claim For Disability Benefits
Complete this form if you became disabled after having been. The attending health care provider shall complete and return to the claimant within seven (7) days of receipt of this form. For approved claims, disability benefits begin on the eighth day of disability. Are you receiving wages, salary or separation pay? Unemployed for more than four (4) weeks.
Form Db 450 Disability ≡ Fill Out Printable PDF Forms Online
For approved claims, disability benefits begin on the eighth day of disability. Notice and proof of claim for disability benefits: For the period of disability covered by this claim: Pfl 1 & 2 forms Mailing address (street & apt.
Form Db450 Notice And Proof Of Claim For Disability Benefits
Complete this form if you became disabled after having been. Web any employee receiving or entitled to receive social security retirement benefits may submit this form at any time to waive any and all benefits under the disability and paid family leave benefits law: The attending health care provider shall complete and return to the claimant within seven (7) days.
Form DB450C Download Fillable PDF or Fill Online Notice and Proof of
Are you receiving or claiming: Mailing address (street & apt. Complete this paperwork if you were working no less than four weeks before the start date of your medical event to apply for benefit payments. The attending health care provider shall complete and return to the claimant within seven (7) days of receipt of this form. The health care provider's.
Unemployed For More Than Four (4) Weeks.
The attending health care provider shall complete and return to the claimant within seven (7) days of receipt of this form. Are you receiving or claiming: The health care provider's statement must be filled in completely. Use this form only when the claimant becomes sick or disabled while employed or becomes sick or disabled within four (4) weeks after termination of employment.
Complete This Paperwork If You Were Working No Less Than Four Weeks Before The Start Date Of Your Medical Event To Apply For Benefit Payments.
Are you receiving wages, salary or separation pay? Complete this form if you became disabled after having been. For the period of disability covered by this claim: Web any employee receiving or entitled to receive social security retirement benefits may submit this form at any time to waive any and all benefits under the disability and paid family leave benefits law:
Mailing Address (Street & Apt.
Notice and proof of claim for disability benefits: Pfl 1 & 2 forms For approved claims, disability benefits begin on the eighth day of disability.