Cms 1763 Printable Form
Cms 1763 Printable Form - 05/21) request for termination of premium hospital and/or supplementary medical insurance. Dates your insurance will end; Try it for free now! Web hi 00820.901 exhibit 1: Try it for free now! People with medicare premium part a or b who would like to terminate their hospital or medical insurance coverage. Web medicare form cms 1763 by ed crowe | agent blog | 0 comment | 10 april, 2020 | medicare form cms 1763 once you decide to terminate your medicare insurance, you need to understand how the process works. The following provides access and/or information for many cms forms. Department of health and human services. Upload, modify or create forms.
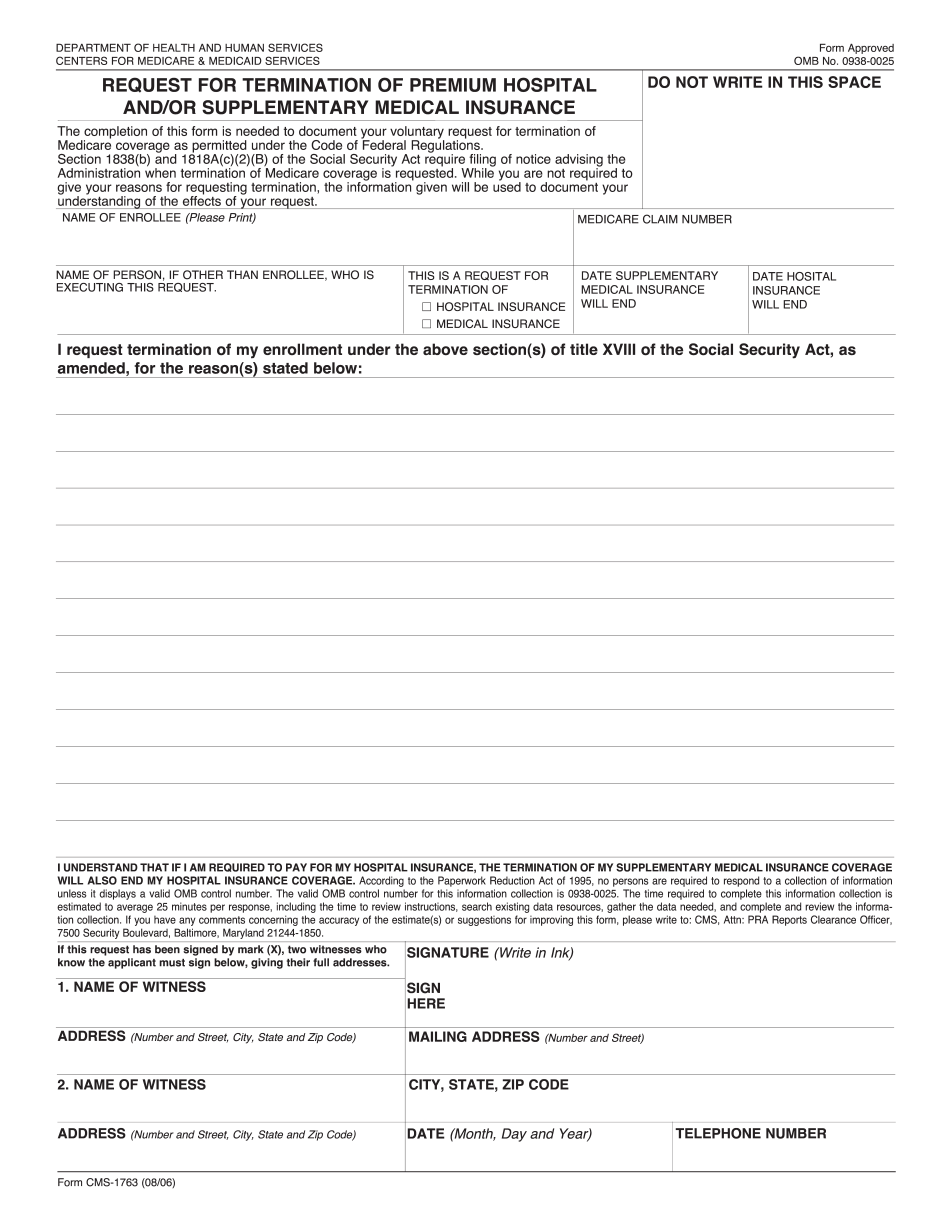
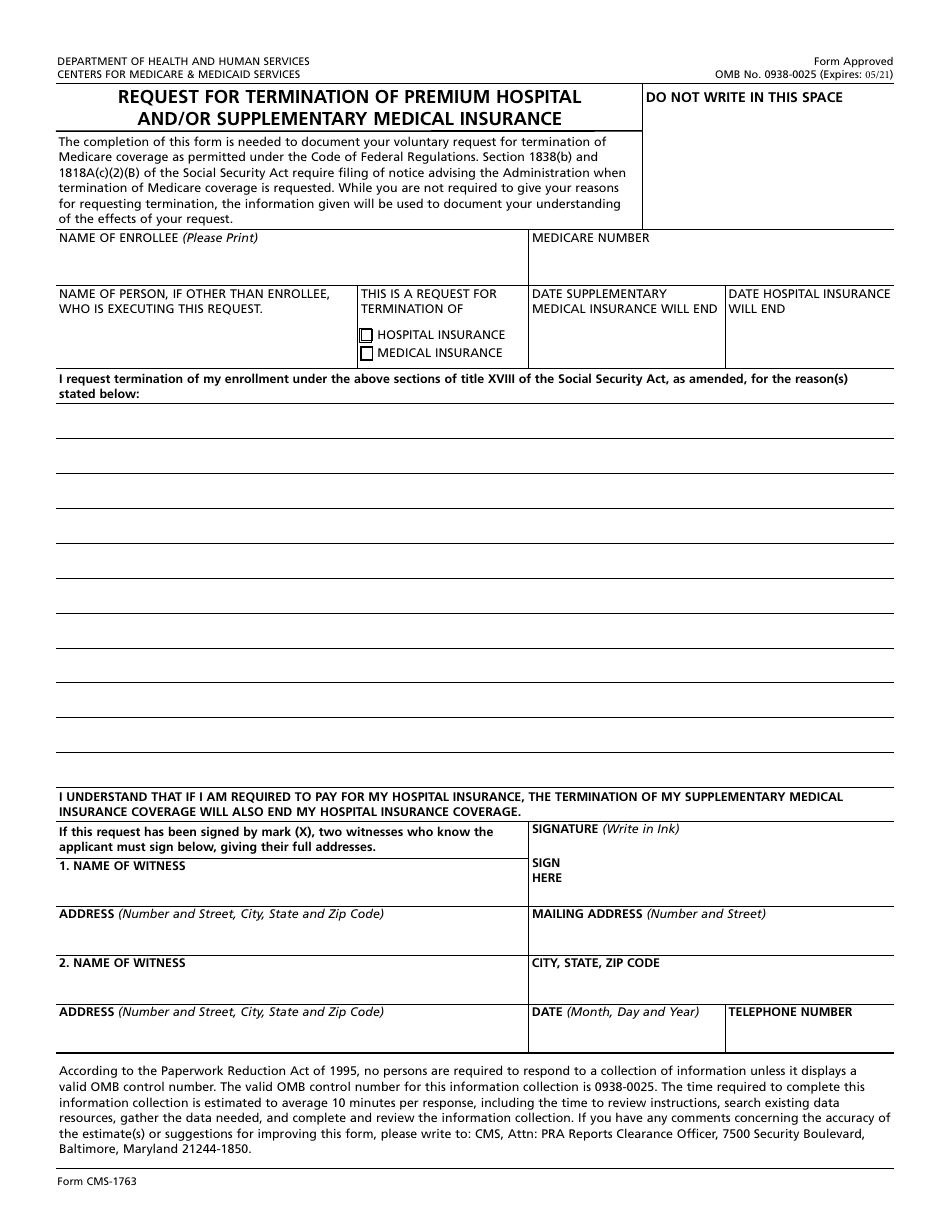
Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. Once completed you can sign your fillable form or send for signing. All forms are printable and downloadable. Web form approved omb no. Try it for free now! Try it for free now! Web the centers for medicare & medicaid services (cms) is a federal agency within the u.s. It consists of the following sections: When do you use this application? 05/21) request for termination of premium hospital and/or supplementary medical insurance.
Upload, modify or create forms. Web the form is relatively simple to fill out. The following provides access and/or information for many cms forms. Many cms program related forms are available in portable document format (pdf). Try it for free now! Exact reasons for the termination; Who can use this form? Upload, modify or create forms. Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. Department of health and human services.
Cms 1763 Fillable, Printable PDF Template
People with medicare premium part a or b who would like to terminate their hospital or medical insurance coverage. Upload, modify or create forms. When do you use this application? Try it for free now! The following provides access and/or information for many cms forms.
Social Security Medicare Form Cms 1763 Form Resume Examples wRYPwQW394
Who can use this form? Try it for free now! Try it for free now! Once completed you can sign your fillable form or send for signing. You may also use the search feature to more quickly locate information for a specific form number or form title.
Gio Workers Compensation Claim Form Nsw Form Resume Template
Dates your insurance will end; Use fill to complete blank online medicare & medicaid pdf forms for free. It consists of the following sections: Upload, modify or create forms. Department of health and human services.
Social Security Medicare Form Cms 1763 Form Resume Examples wRYPwQW394
All forms are printable and downloadable. Exact reasons for the termination; Who can use this form? Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. Enrollee’s name (or a legal representative);

Fill Free fillable Form CMS1763 REQUEST FOR TERMINATION OF PREMIUM
Upload, modify or create forms. Notice of denial of medical coverage/payment (integrated denial notice) All forms are printable and downloadable. Many cms program related forms are available in portable document format (pdf). When do you use this application?

Fill Medicare & Medicaid
Try it for free now! 05/21) request for termination of premium hospital and/or supplementary medical insurance. Dates your insurance will end; Web medicare form cms 1763 by ed crowe | agent blog | 0 comment | 10 april, 2020 | medicare form cms 1763 once you decide to terminate your medicare insurance, you need to understand how the process works..

Printable Medicare Part A Application Form Form Resume Examples
All forms are printable and downloadable. You may also use the search feature to more quickly locate information for a specific form number or form title. Web form approved omb no. Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. Upload, modify or create forms.
Non Social Security 1099 Form Form Resume Examples 1ZV8gPEY3X
Upload, modify or create forms. Try it for free now! Notice of denial of medical coverage/payment (integrated denial notice) Department of health and human services. Web medicare form cms 1763 by ed crowe | agent blog | 0 comment | 10 april, 2020 | medicare form cms 1763 once you decide to terminate your medicare insurance, you need to understand.
Form CMS1763 Download Fillable PDF or Fill Online Request for
Web cms forms list. Web the form is relatively simple to fill out. Web hi 00820.901 exhibit 1: It consists of the following sections: Many cms program related forms are available in portable document format (pdf).
Where Do I Mail Medicare Form Cms 1763 Form Resume Examples AjYdXvKoYl
First, you will need to fill out a medicare form cms 1763. The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of. People with medicare premium part a or b who would like to terminate their hospital or medical insurance coverage. Enrollee’s name (or a legal representative);.
It Consists Of The Following Sections:
Web hi 00820.901 exhibit 1: Web form approved omb no. Upload, modify or create forms. Try it for free now!
Many Cms Program Related Forms Are Available In Portable Document Format (Pdf).
Who can use this form? The following provides access and/or information for many cms forms. Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. Web medicare form cms 1763 by ed crowe | agent blog | 0 comment | 10 april, 2020 | medicare form cms 1763 once you decide to terminate your medicare insurance, you need to understand how the process works.
People With Medicare Premium Part A Or B Who Would Like To Terminate Their Hospital Or Medical Insurance Coverage.
Notice of denial of medical coverage/payment (integrated denial notice) Upload, modify or create forms. 05/21) request for termination of premium hospital and/or supplementary medical insurance. Use fill to complete blank online medicare & medicaid pdf forms for free.
Department Of Health And Human Services.
Try it for free now! Dates your insurance will end; Web cms forms list. The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of.