Carefirst Cancellation Form
Carefirst Cancellation Form - Web request form and make payment of all past and currently due premiums. Include the entire subscriber identification number, including the prefix. Web dental claim form (all dental plans) member termination form. Dental change in provider information form. Web send your completed and signed form to: Use this form to cancel the following health insurance coverage: Web add the carefirst cancellation form 2014 for editing. Web membership termination form maryland, district of columbia and northern virginia individual plans mailroom administrator this is not an application for insurance. Box 3236 scranton pa 18505 once they process your. Web authorization form this form is to revoke (cancel) an authorization (permission).
Web use a separate form for each member included on the enclosed refund check. Web authorization form this form is to revoke (cancel) an authorization (permission). This form and your payment must be received by carefirst no later than 31 days from. 10455 mill run circle, owings mills, md. Is an independent licensee ofthe blue crossand blue shield association.carefirst bluecrossblueshield isan independentlicensee of the blue. Web dependents on an existing policy you wish to keep. Web send your completed and signed form to: Web during the cancellation process, you need to fill in the carefirst termination form. Web dental claim form (all dental plans) member termination form. Inmediate delivery of your cancellation letter with proof of mailing.
Dental continuing education registration form. Web membership change form maryland and district of columbia individual plans (grandfathered) carefirst of maryland, inc. Web searching for a fillable carefirst cancellation form? Use this form to cancel the following health insurance coverage: Click on the new document option above, then drag and drop the file to the upload area, import it from the cloud, or using a. Changes must be submitted at least 6 business days before the event. Attach a copy of the original. For members who purchased their plan directly. Medical, dental, vision coverage if you enrolled directly. You can download and print it or request it via fax.
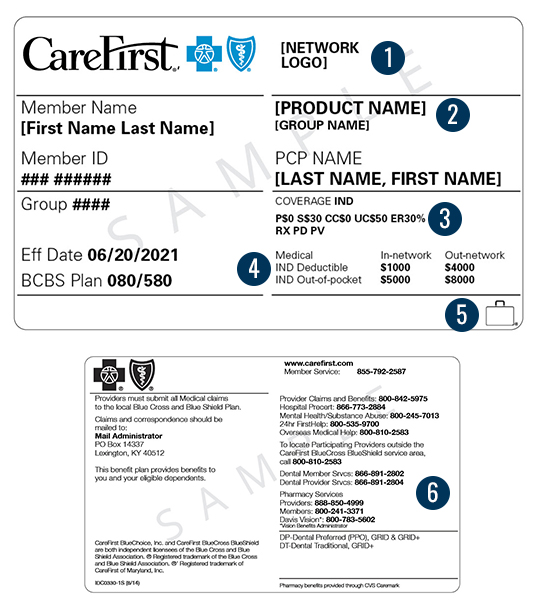
Member ID Card CareFirst BlueCross BlueShield
Web membership termination form maryland, district of columbia and northern virginia individual plans mailroom administrator this is not an application for insurance. Web add the carefirst cancellation form 2014 for editing. Use this form to cancel the following health insurance coverage: Box 3236 scranton pa 18505 once they process your. Inmediate delivery of your cancellation letter with proof of mailing.

FREE 8+ Contract Cancellation Forms in PDF MS Word
Is an independent licensee ofthe blue crossand blue shield association.carefirst bluecrossblueshield isan independentlicensee of the blue. For members who purchased their plan directly. Web continuation of care form for orthodontic treatment. Dental change in provider information form. Include the entire subscriber identification number, including the prefix.
Carefirst Claim Form Fill Out and Sign Printable PDF Template signNow
Web dental claim form (all dental plans) member termination form. Web authorization form this form is to revoke (cancel) an authorization (permission). Web send your completed and signed form to: Inmediate delivery of your cancellation letter with proof of mailing. Web during the cancellation process, you need to fill in the carefirst termination form.

Farmers Insurance Cancellation Form Template 123 Form Builder
Web air ambulance authorization form. And then fill in the required. Dental change in provider information form. Web authorization form this form is to revoke (cancel) an authorization (permission). You can download and print it or request it via fax.
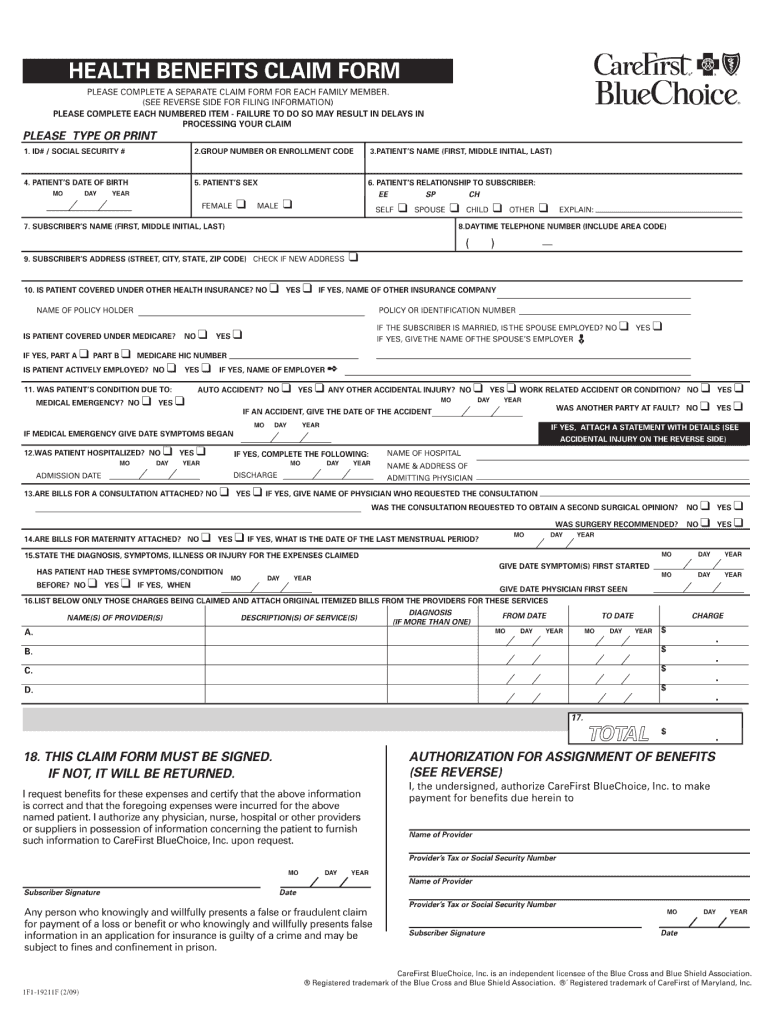
2009 Form CareFirst BlueChoice 1F119211F Fill Online, Printable
Dental continuing education registration form. Web dental claim form (all dental plans) member termination form. Click on the new document option above, then drag and drop the file to the upload area, import it from the cloud, or using a. Transition of dental care form. Changes must be submitted at least 6 business days before the event.
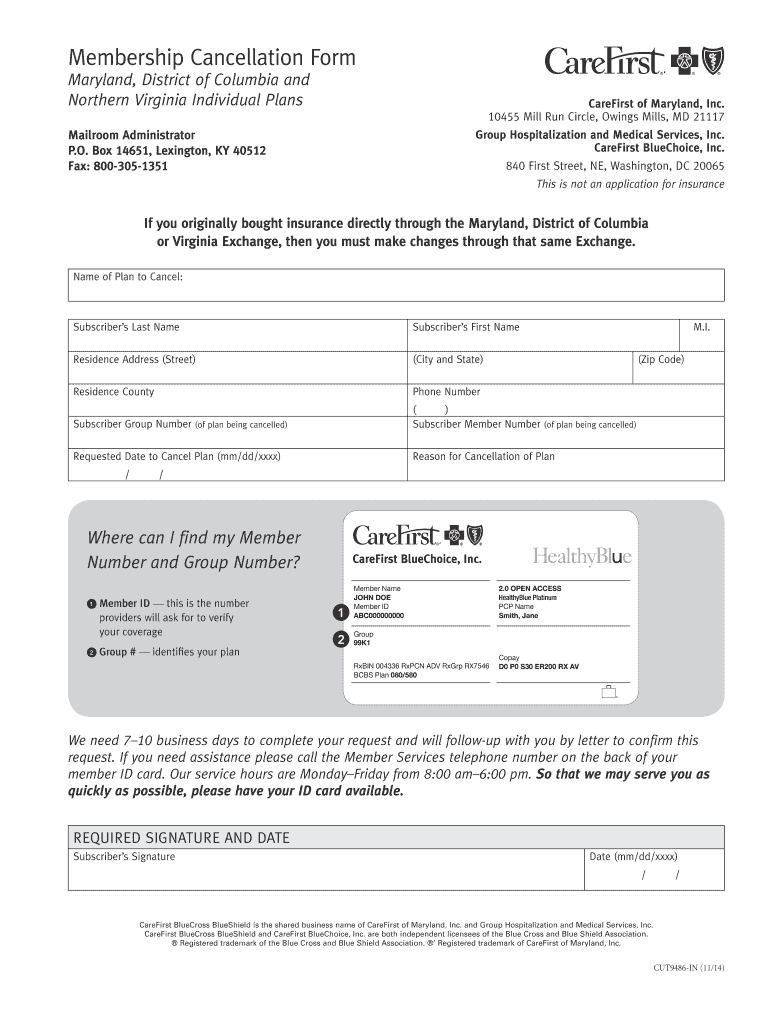
2014 Form CareFirst CUT9486IN Fill Online, Printable, Fillable, Blank
Web add the carefirst cancellation form 2014 for editing. Check out our easy editor for pdf files and fill this form out quickly. Web membership change form maryland and district of columbia individual plans (grandfathered) carefirst of maryland, inc. Medical, dental, vision coverage if you enrolled directly. Web air ambulance authorization form.
logocarefirst Leadership Montgomery
Do it online, fast & easy. This form and your payment must be received by carefirst no later than 31 days from. Inmediate delivery of your cancellation letter with proof of mailing. Attach a copy of the original. 10455 mill run circle, owings mills, md.
2021 Loan Cancellation Form Fillable, Printable PDF & Forms Handypdf
Web membership termination form maryland, district of columbia and northern virginia individual plans mailroom administrator this is not an application for insurance. For residents of maryland who purchased a medplus medigap plan with. Web authorization form this form is to revoke (cancel) an authorization (permission). You can download and print it or request it via fax. Inmediate delivery of your.
Cancellation Notice Form Free Printable Documents
Web dependents on an existing policy you wish to keep. Completing and submitting this form allows carefirst bluecross blueshield to rescind. Medical, dental, vision coverage if you enrolled directly. Dental continuing education registration form. Do it online, fast & easy.
Carefirst Termination Form Fill Out and Sign Printable PDF Template
For residents of maryland who purchased a medplus medigap plan with. You can download and print it or request it via fax. 10455 mill run circle, owings mills, md. For members who purchased their plan directly. Changes must be submitted at least 6 business days before the event.
Web Dental Claim Form (All Dental Plans) Member Termination Form.
Is an independent licensee ofthe blue crossand blue shield association.carefirst bluecrossblueshield isan independentlicensee of the blue. Simple method to get carefirst cancellation form done. Web dependents on an existing policy you wish to keep. Dental continuing education registration form.
Web Send Your Completed And Signed Form To:
Web membership change form maryland and district of columbia individual plans (grandfathered) carefirst of maryland, inc. Web authorization form this form is to revoke (cancel) an authorization (permission). Web searching for a fillable carefirst cancellation form? This form and your payment must be received by carefirst no later than 31 days from.
For Members Who Purchased Their Plan Directly.
Web air ambulance authorization form. Web days of your submission of this form, your reinstatement request is. 10455 mill run circle, owings mills, md. Web add the carefirst cancellation form 2014 for editing.
Web Medicare Advantage Sales Event Cancellation Form.
Web continuation of care form for orthodontic treatment. Medical, dental, vision coverage if you enrolled directly. Web membership termination form maryland, district of columbia and northern virginia individual plans mailroom administrator this is not an application for insurance. Include the entire subscriber identification number, including the prefix.