Blue Cross Blue Shield Cancellation Form
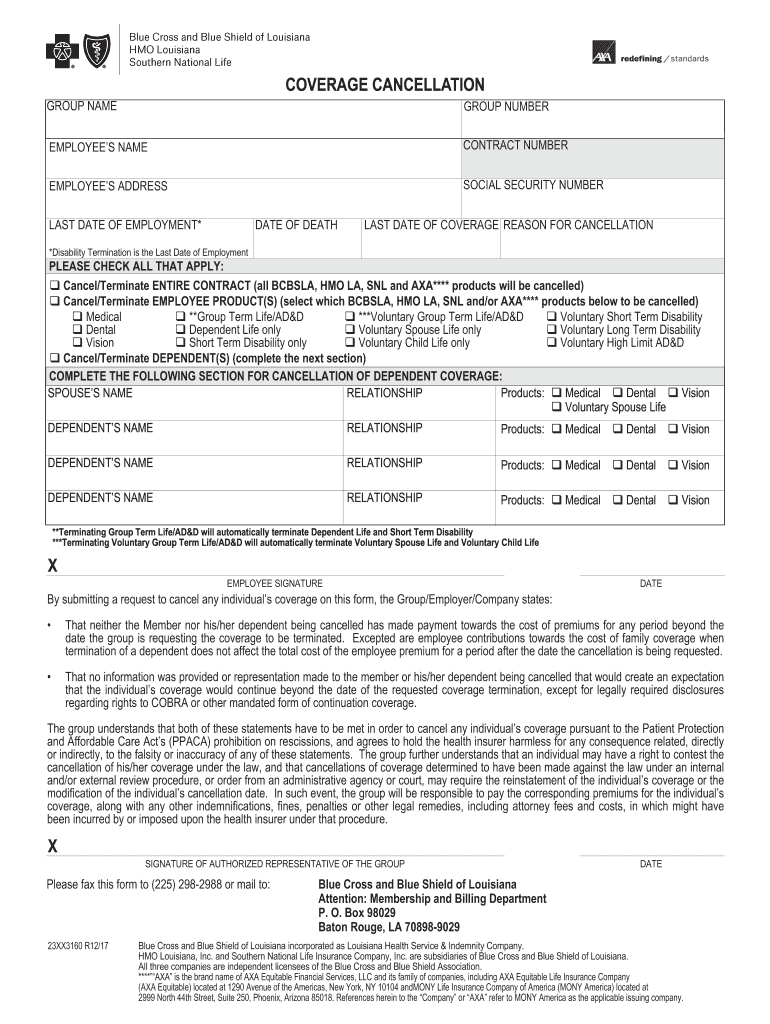
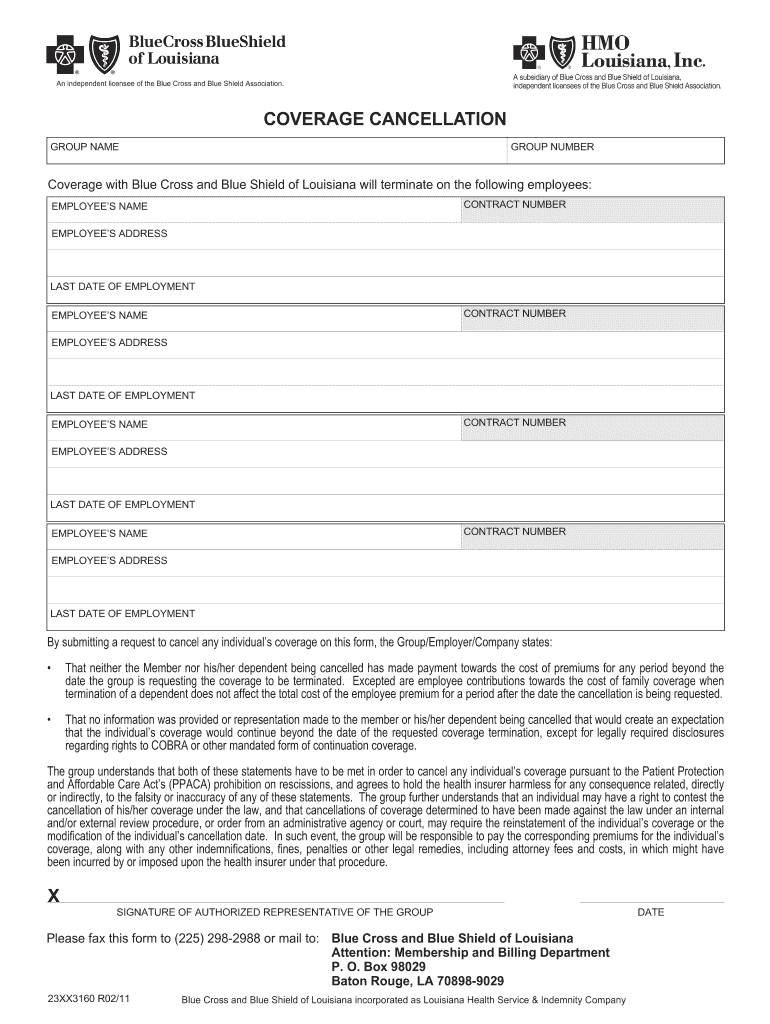
Blue Cross Blue Shield Cancellation Form - Blue cross and blue shield of minnesota, p.o. Cancellation requests must reach the blue cross blue shield office before the first of the month of the requested cancellation date, and must be. Policy number/member id member’s name cancellation date current date (date of request) subscriber’s signature. Web talk to a health plan consultant: Individual plan cancellation form (death of policyholder) individual plan cancellation form (death of policyholder) (spanish). Web coverage of handicapped dependent child application *. Web forms and documents for individuals and families. Web cancel all dependent coverage only cancel coverage only on the dependent(s) listed below in section c reason for cancellation: This form is used to cancel a policy. Web involuntary disenrollment there are times when the plan must disenroll a member:
Web talk to a health plan consultant: Web cancel all dependent coverage only cancel coverage only on the dependent(s) listed below in section c reason for cancellation: Web cancel blue cross blue shield. Web to enroll, reenroll, or to elect not to enroll in the fehb program, or to change, cancel or suspend your fehb enrollment please complete and file this form. Web indian health service referral form. Web involuntary disenrollment there are times when the plan must disenroll a member: Blue cross blue shield of michigan general member claim form. Cancellation requests must reach the blue cross blue shield office before the first of the month of the requested cancellation date, and must be. Box 982801, el paso, tx 79998 fax to: Web forms and documents for individuals and families.
Coverage by mail, take the following steps: Your membership in our plan will end on the last day of the month in which your disenrollment request notice is received. Blue cross blue shield of michigan general member claim form. Web if you purchase insurance individually (not through an employer) and need to make a change, please call us at 800‑280‑2583. Web involuntary disenrollment there are times when the plan must disenroll a member: Web forms and documents for individuals and families. Individual plan cancellation form (death of policyholder) individual plan cancellation form (death of policyholder) (spanish). Web talk to a health plan consultant: Left employment retired reduction of work hours. If you get your insurance through work, please.
How to File Blue Cross Blue Shield Overseas Medical Claims YouMeMindBody
Web coverage of handicapped dependent child application *. Access all the forms and documents you need to manage your health plan—from claims forms to health information. The individual moves out of the plan’s service area and becomes ineligible to be an enrollee. Your membership in our plan will end on the last day of the month in which your disenrollment.

Blue Cross Blue Shield Truscott Rossman
Register now, or download the sydney health. Web indian health service referral form. This form is used to cancel a policy. Web cancel blue cross blue shield. Blue cross and blue shield of minnesota, p.o.

Bluecross Blue Shield Kamasutra Porn Videos
Web the request must be a statement that includes: Blue cross blue shield of michigan general member claim form. Web cancel blue cross blue shield. Web cancel all dependent coverage only cancel coverage only on the dependent(s) listed below in section c reason for cancellation: Left employment retired reduction of work hours.

Avoiding Vision Loss from Diabetes Blue Cross and Blue Shield of Montana
Use this form to manually submit a claim for a medical, vision or hearing service if you're a blue. Web the request must be a statement that includes: Individual plan cancellation form (death of policyholder) individual plan cancellation form (death of policyholder) (spanish). Coverage by mail, take the following steps: Web cancel blue cross blue shield.
Florida Blue Cancellation Form Fill Out and Sign Printable PDF
Access all the forms and documents you need to manage your health plan—from claims forms to health information. Web indian health service referral form. Web cancellation of a policy at the request of the policyholder or an agent will be done on the 1st or the 15th (depending on the billing cycle) following receipt of a signed. Web coverage of.
Blue Cross Blue Shield Cancellation Form Fill Out and Sign Printable
Web cancel all dependent coverage only cancel coverage only on the dependent(s) listed below in section c reason for cancellation: Web cancellation of a policy at the request of the policyholder or an agent will be done on the 1st or the 15th (depending on the billing cycle) following receipt of a signed. Web indian health service referral form. Web.

Blue Cross Blue Shield Cancellation Form Fill Online, Printable
Web cancel blue cross blue shield. Left employment retired reduction of work hours. Blue cross blue shield of michigan general member claim form. Access all the forms and documents you need to manage your health plan—from claims forms to health information. Your membership in our plan will end on the last day of the month in which your disenrollment request.
Thank you, Blue Cross and Blue Shield!Supportive Housing Coalition
Policy number/member id member’s name cancellation date current date (date of request) subscriber’s signature. Blue cross blue shield of michigan general member claim form. Fill out the cancellation form in blue or black ink with legible. Web coverage of handicapped dependent child application *. Web talk to a health plan consultant:

Blue Cross Blue Shield Settlement Details BerniePortal
Your membership in our plan will end on the last day of the month in which your disenrollment request notice is received. Web forms and documents for individuals and families. Fill out the cancellation form in blue or black ink with legible. Individual plan cancellation form (death of policyholder) individual plan cancellation form (death of policyholder) (spanish). Access all the.

Blue Cross Blue Shield ACA rates going up in 2018 ABC11 RaleighDurham
Web involuntary disenrollment there are times when the plan must disenroll a member: Individual plan cancellation form (death of policyholder) individual plan cancellation form (death of policyholder) (spanish). Access all the forms and documents you need to manage your health plan—from claims forms to health information. Web to enroll, reenroll, or to elect not to enroll in the fehb program,.
Web The Request Must Be A Statement That Includes:
Web cancellation of a policy at the request of the policyholder or an agent will be done on the 1st or the 15th (depending on the billing cycle) following receipt of a signed. Web cancel all dependent coverage only cancel coverage only on the dependent(s) listed below in section c reason for cancellation: Access all the forms and documents you need to manage your health plan—from claims forms to health information. Use this form to manually submit a claim for a medical, vision or hearing service if you're a blue.
Web Talk To A Health Plan Consultant:
The individual moves out of the plan’s service area and becomes ineligible to be an enrollee. Web forms and documents for individuals and families. Fill out the cancellation form in blue or black ink with legible. Cancellation requests must reach the blue cross blue shield office before the first of the month of the requested cancellation date, and must be.
Policy Number/Member Id Member’s Name Cancellation Date Current Date (Date Of Request) Subscriber’s Signature.
Web if you purchase insurance individually (not through an employer) and need to make a change, please call us at 800‑280‑2583. Blue cross blue shield of michigan general member claim form. Your membership in our plan will end on the last day of the month in which your disenrollment request notice is received. Web cancel blue cross blue shield.
Web Indian Health Service Referral Form.
Blue cross and blue shield of minnesota, p.o. Web to enroll, reenroll, or to elect not to enroll in the fehb program, or to change, cancel or suspend your fehb enrollment please complete and file this form. Web coverage of handicapped dependent child application *. This form is used to cancel a policy.