Ambetter Prior Authorization Form Pdf
Ambetter Prior Authorization Form Pdf - Or fax this completed form to 866.399.0929 envolve pharmacy solutions and ambetter will respond via fax or phone within 24 hours of receipt of all necessary information, except during weekends or holidays. Member id * last name,. When we receive your prior authorization request, our nurses and doctors will review it. Use your zip code to find your personal plan. Prior authorization guide (pdf) inpatient prior authorization fax form (pdf) outpatient prior authorization fax form (pdf) provider fax back form (pdf) mo marketplace out of network form (pdf) ambetter from home state health oncology pathway solutions faqs (pdf) national imaging associates, inc. Copies of all supporting clinical information are required. Find and enroll in a plan that's right for you. Web services must be a covered benefit and medically necessary with prior authorization as per ambetter policy and procedures. Join ambetter show join ambetter menu To see if a service requires authorization, check with your primary care provider (pcp), the ordering provider or member services.
Or fax this completed form to 866.399.0929 envolve pharmacy solutions and ambetter will respond via fax or phone within 24 hours of receipt of all necessary information, except during weekends or holidays. Web this process is known as prior authorization. Yes no ☐ ☐ ☐ therapy status: Servicing provider / facility information. Same as requesting provider servicing. Member id * last name,. Web services must be a covered benefit and medically necessary with prior authorization as per ambetter policy and procedures. Join ambetter show join ambetter menu The information contained in this transmission is confidential and may be protected under the health insurance portability and accountability act of 1996. ☐ initial ☐ continuation if continuation, provide therapy start date:
☐ initial ☐ continuation if continuation, provide therapy start date: Yes no ☐ ☐ ☐ therapy status: Web services must be a covered benefit and medically necessary with prior authorization as per ambetter policy and procedures. Copies of all supporting clinical information are required. Member id * last name,. The information contained in this transmission is confidential and may be protected under the health insurance portability and accountability act of 1996. See coverage in your area; Prior authorization guide (pdf) inpatient prior authorization fax form (pdf) outpatient prior authorization fax form (pdf) provider fax back form (pdf) mo marketplace out of network form (pdf) ambetter from home state health oncology pathway solutions faqs (pdf) national imaging associates, inc. Servicing provider / facility information. When we receive your prior authorization request, our nurses and doctors will review it.

FREE 11+ Prior Authorization Forms in PDF MS Word
Join ambetter show join ambetter menu Web visit covermymeds.com/epa/envolverx to begin using this free service. Web services must be a covered benefit and medically necessary with prior authorization as per ambetter policy and procedures. Same as requesting provider servicing. Member id * last name,.
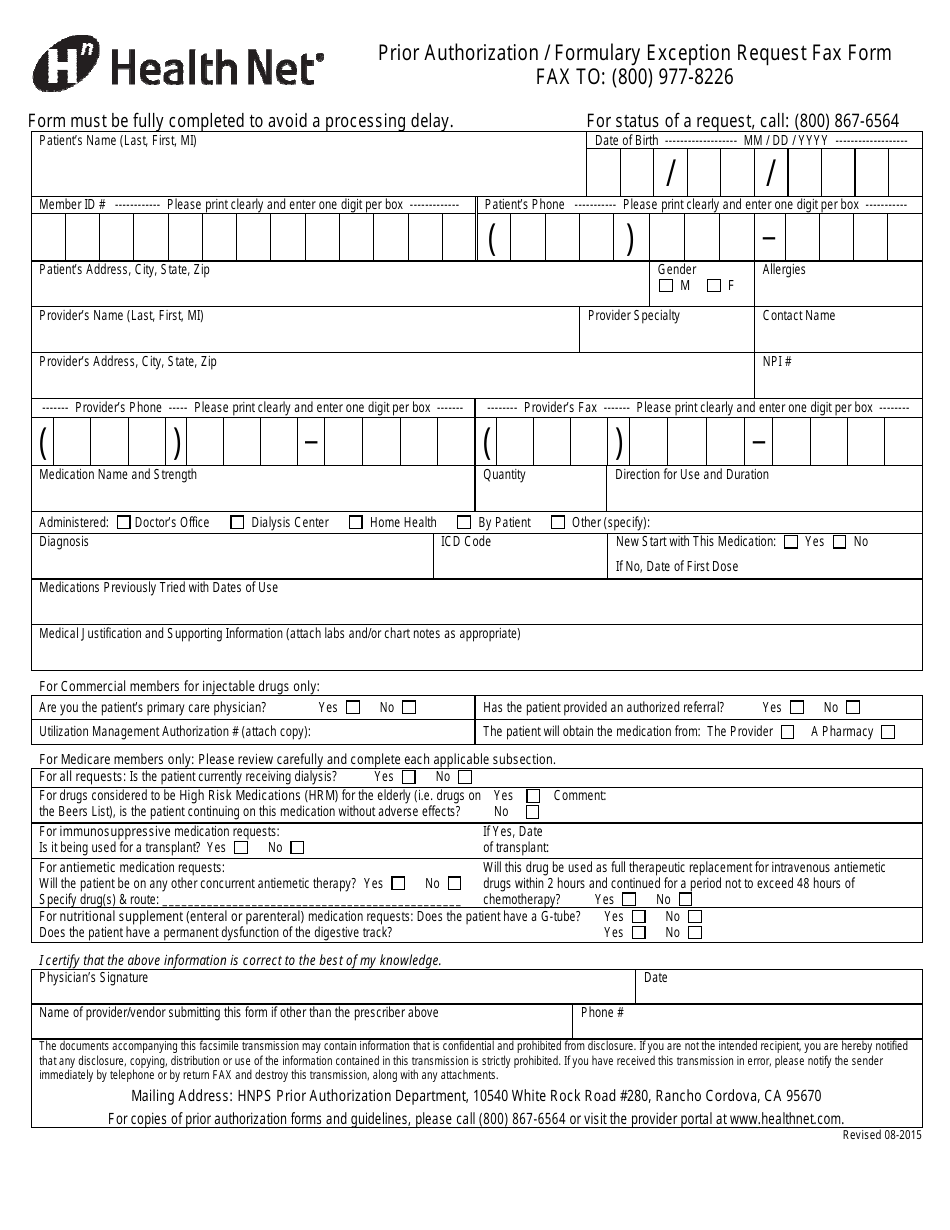
Prior Authorization/Formulary Exception Request Fax Form Health Net
Same as requesting provider servicing. Web visit covermymeds.com/epa/envolverx to begin using this free service. Web services must be a covered benefit and medically necessary with prior authorization as per ambetter policy and procedures. Copies of all supporting clinical information are required. See coverage in your area;

Gallery of Ambetter Prior Authorization form Beautiful Kircblog 2015
Web prior authorization fax form fax to: Web inpatient prior authorization fax form (pdf) outpatient prior authorization fax form (pdf) change of provider request form (pdf) transcranial magnetic stimulation services prior authorization checklist (pdf) psychological and neuropsychological testing checklist (pdf) electroconvulsive therapy (ect) checklist (pdf) ambetter behavioral health. All required fields must be filled in as incomplete forms will be.

Gallery of Ambetter Prior Authorization form Beautiful Kircblog 2015
Copies of all supporting clinical information are required. Use your zip code to find your personal plan. Yes no ☐ ☐ ☐ therapy status: Web this process is known as prior authorization. All required fields must be filled in as incomplete forms will be rejected.

Gallery of Ambetter Prior Authorization form Beautiful Kircblog 2015
Web visit covermymeds.com/epa/envolverx to begin using this free service. See coverage in your area; Prior authorization guide (pdf) inpatient prior authorization fax form (pdf) outpatient prior authorization fax form (pdf) provider fax back form (pdf) mo marketplace out of network form (pdf) ambetter from home state health oncology pathway solutions faqs (pdf) national imaging associates, inc. Web this process is.

Medicare Part D Medco Prior Authorization Form Printable
Web prior authorization fax form fax to: Yes no ☐ ☐ ☐ therapy status: To see if a service requires authorization, check with your primary care provider (pcp), the ordering provider or member services. Prior authorization guide (pdf) inpatient prior authorization fax form (pdf) outpatient prior authorization fax form (pdf) provider fax back form (pdf) mo marketplace out of network.
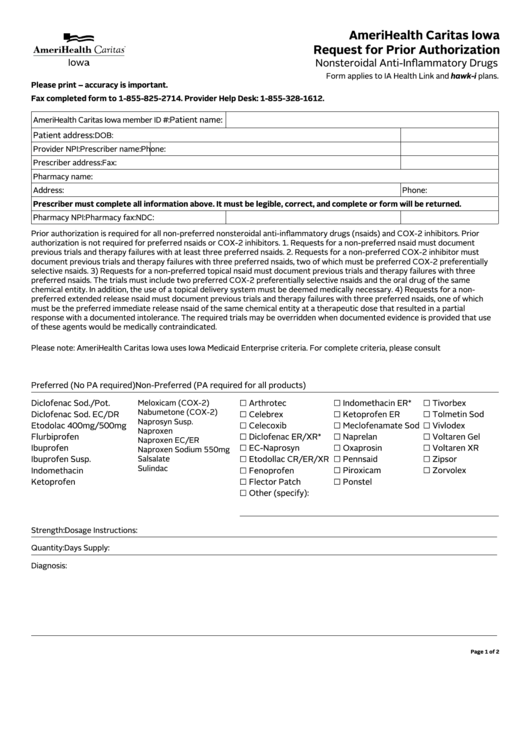
Fillable Request For Prior Authorization Form printable pdf download
Web inpatient prior authorization fax form (pdf) outpatient prior authorization fax form (pdf) change of provider request form (pdf) transcranial magnetic stimulation services prior authorization checklist (pdf) psychological and neuropsychological testing checklist (pdf) electroconvulsive therapy (ect) checklist (pdf) ambetter behavioral health. Use your zip code to find your personal plan. Or fax this completed form to 866.399.0929 envolve pharmacy solutions.
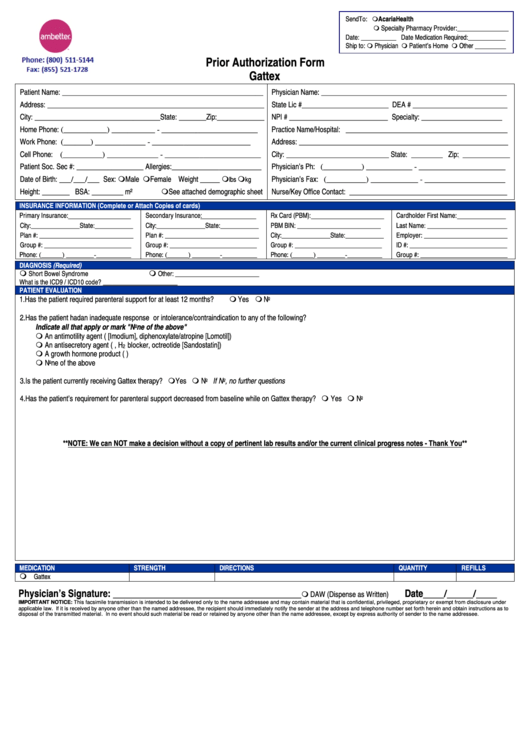
Ambetter Prior Authorization Form Gattex printable pdf download
Find and enroll in a plan that's right for you. ☐ initial ☐ continuation if continuation, provide therapy start date: Web visit covermymeds.com/epa/envolverx to begin using this free service. Use your zip code to find your personal plan. All required fields must be filled in as incomplete forms will be rejected.

Gallery of Ambetter Prior Authorization form Beautiful Kircblog 2015
Or fax this completed form to 866.399.0929 envolve pharmacy solutions and ambetter will respond via fax or phone within 24 hours of receipt of all necessary information, except during weekends or holidays. To see if a service requires authorization, check with your primary care provider (pcp), the ordering provider or member services. Yes no ☐ ☐ ☐ therapy status: See.
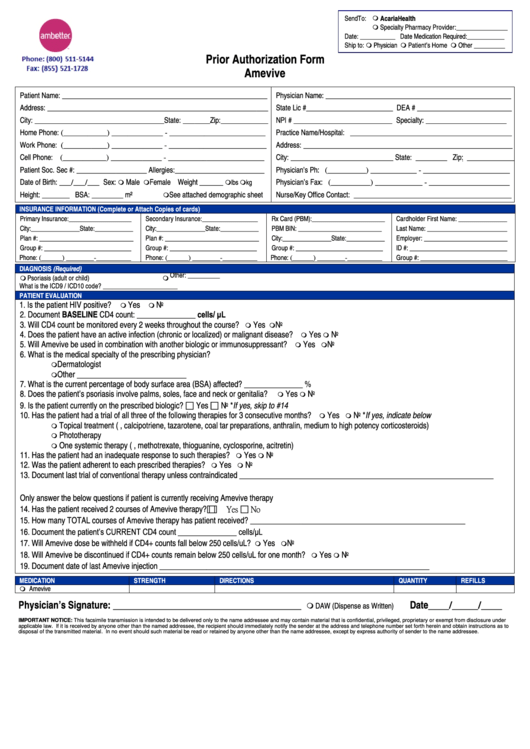
Ambetter Prior Authorization Form Amevive printable pdf download
Servicing provider / facility information. Web prior authorization fax form fax to: See coverage in your area; Same as requesting provider servicing. Web inpatient prior authorization fax form (pdf) outpatient prior authorization fax form (pdf) change of provider request form (pdf) transcranial magnetic stimulation services prior authorization checklist (pdf) psychological and neuropsychological testing checklist (pdf) electroconvulsive therapy (ect) checklist (pdf).
All Required Fields Must Be Filled In As Incomplete Forms Will Be Rejected.
Find and enroll in a plan that's right for you. Web visit covermymeds.com/epa/envolverx to begin using this free service. When we receive your prior authorization request, our nurses and doctors will review it. Web prior authorization fax form fax to:
☐ Initial ☐ Continuation If Continuation, Provide Therapy Start Date:
Join ambetter show join ambetter menu Prior authorization guide (pdf) inpatient prior authorization fax form (pdf) outpatient prior authorization fax form (pdf) provider fax back form (pdf) mo marketplace out of network form (pdf) ambetter from home state health oncology pathway solutions faqs (pdf) national imaging associates, inc. Drug information drug name and strength: Web services must be a covered benefit and medically necessary with prior authorization as per ambetter policy and procedures.
Servicing Provider / Facility Information.
Use your zip code to find your personal plan. Web this process is known as prior authorization. Or fax this completed form to 866.399.0929 envolve pharmacy solutions and ambetter will respond via fax or phone within 24 hours of receipt of all necessary information, except during weekends or holidays. Copies of all supporting clinical information are required.
Lack Of Clinical Information May Result In Delayed Determination.
Member id * last name,. Yes no ☐ ☐ ☐ therapy status: Same as requesting provider servicing. See coverage in your area;