Aetna Reconsideration Form For Providers
Aetna Reconsideration Form For Providers - How do i submit requests for reconsideration online? Web your claim reconsideration must include this completed form and any additional information (proof from primary payer, required documentation, cms or medicaid. Sign it in a few clicks draw your signature, type. Web please complete this form if you are seeking reconsideration of a previous billing determination. Web forms for health care professionals find all the forms you need find forms and applications for health care professionals and patients, all in one place. Be specific when completing the description of dispute and. Web appeals must be submitted by mail/fax, using the provider complaint and appeal form. Web provider info provider network files these links provides access to our aetna better health of texas provider directory xml files which can be downloaded by third parties and. To obtain a review submit this form as. Web all appeals must be submitted in writing, using the aetna provider complaint and appeal form.
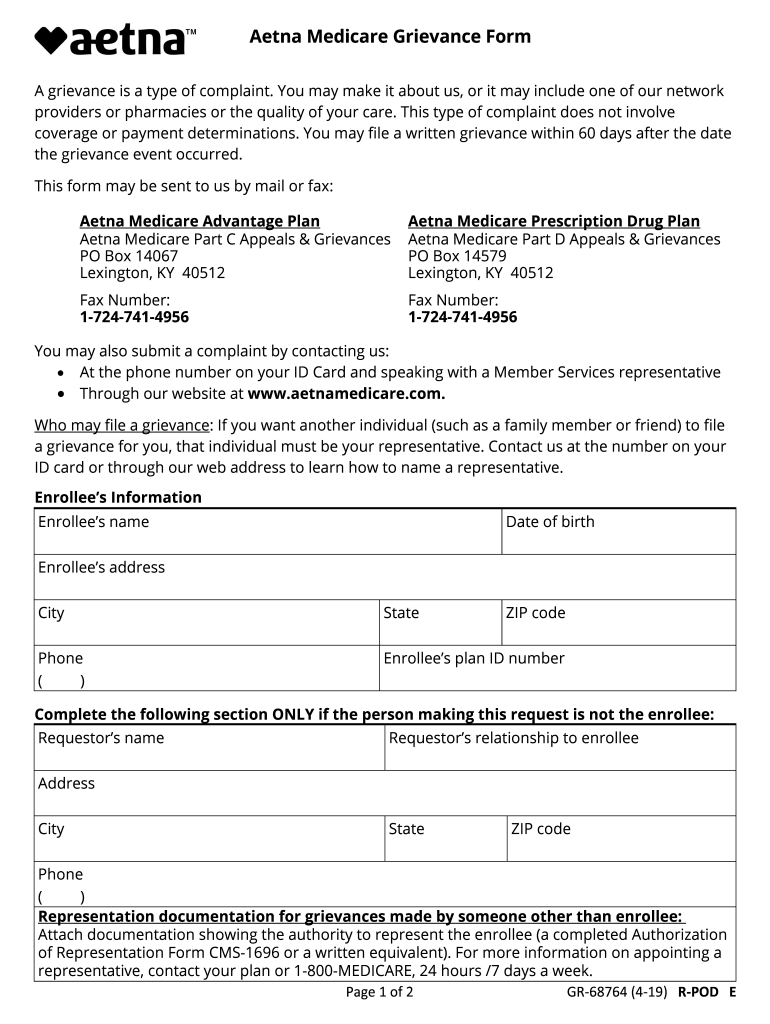
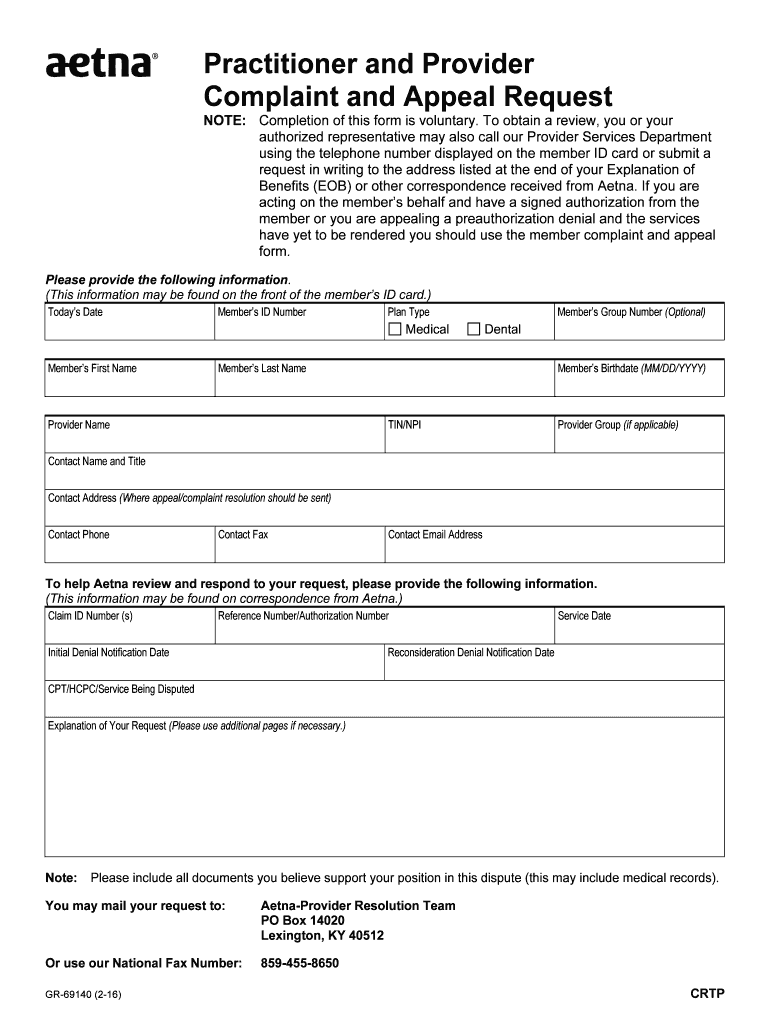
Sign it in a few clicks draw your signature, type. Within 180 calendar days of the initial claim decision. Explanation of your request (please use additional pages if necessary.) you may mail. Web if you have a dispute around a payment you would have received under original medicare please send your dispute, documentation of what original medicare. Web reconsideration denial notification date(s) cpt/hcpc/service being disputed. Web medical dental member’s first name member’s last name member’s birthdate (mm/dd/yyyy) tohelp usreviewand respond to your request, please providethefollowing. To obtain a review submit this form as. How do i submit requests for reconsideration online? Web a reconsideration is a formal review of a previous claim reimbursement or coding decision, or a claim that requires reprocessing where the denial is not based on medical necessity. Web your claim reconsideration must include this completed form and any additional information (proof from primary payer, required documentation, cms or medicaid.
Explanation of your request (please use additional pages if necessary.) you may mail. Reconsideration denial notification date(s) cpt/hcpc/service being disputed. To obtain a review submit this form as. Be specific when completing the description of dispute and. Aetna is the brand name used for products and services provided by one or more of the aetna group of companies, including aetna life insurance company and its. Completion of this form is mandatory. Within 180 calendar days of the initial claim decision. Web appeals must be submitted by mail/fax, using the provider complaint and appeal form. Web medical dental member’s first name member’s last name member’s birthdate (mm/dd/yyyy) tohelp usreviewand respond to your request, please providethefollowing. Web if you have a dispute around a payment you would have received under original medicare please send your dispute, documentation of what original medicare.

Aetna Provider Claim Resubmission Reconsideration form Best Of Appeal
Web please complete this form if you are seeking reconsideration of a previous billing determination. Web appeals must be submitted by mail/fax, using the provider complaint and appeal form. Get a provider complaint and appeal form (pdf) to facilitate handling: Web provider appeals dispute & appeal process: Edit your appeals from aetna online type text, add images, blackout confidential details,.

Aetna Appeal Letter Sample Templates
Be specific when completing the description of dispute and. Web please complete this form if you are seeking reconsideration of a previous billing determination. Within 180 calendar days of the initial claim decision. To obtain a review submit this form as. Web reconsideration denial notification date(s) cpt/hcpc/service being disputed.

ads/responsive.txt Aetna Provider Claim Resubmission Reconsideration
Web claims reconsideration & appeals form complete this form and return to aetna better health of texas for processing your request. Completion of this form is mandatory. Web your claim reconsideration must include this completed form and any additional information (proof from primary payer, required documentation, cms or medicaid. Web provider appeals dispute & appeal process: Web please complete this.
Aetna Medicare Complaint Team Fill Out and Sign Printable PDF
Get a provider complaint and appeal form (pdf) to facilitate handling: Web claims reconsideration & appeals form complete this form and return to aetna better health of texas for processing your request. Web provider info provider network files these links provides access to our aetna better health of texas provider directory xml files which can be downloaded by third parties.
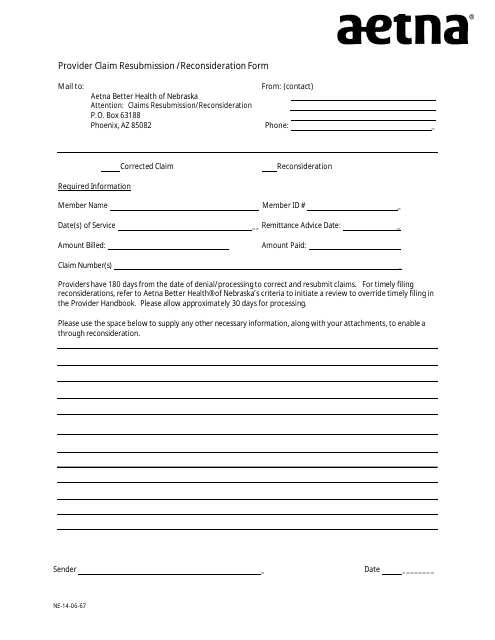
Nebraska Provider Claim Resubmission/Reconsideration Form Aetna
How do i submit requests for reconsideration online? To obtain a review submit this form as. Web a reconsideration is a formal review of a previous claim reimbursement or coding decision, or a claim that requires reprocessing where the denial is not based on medical necessity. Completion of this form is mandatory. Web please complete this form if you are.
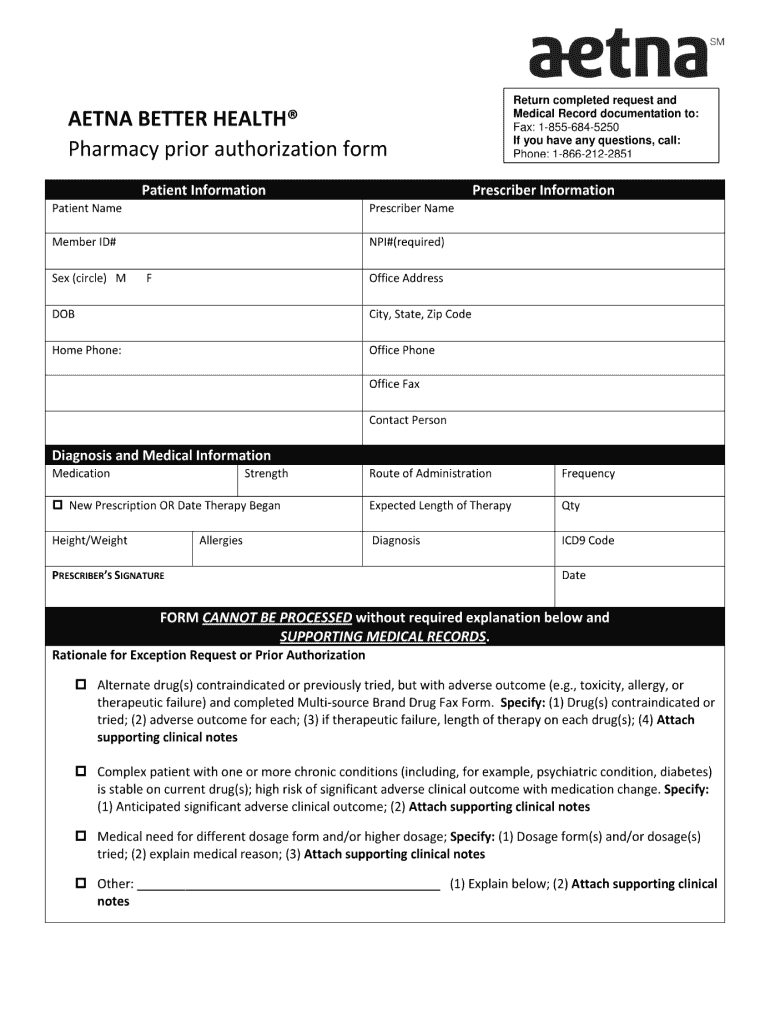
Aetna Prior Authorization Form Pdf Fill Out and Sign Printable PDF
Web medical dental member’s first name member’s last name member’s birthdate (mm/dd/yyyy) tohelp usreviewand respond to your request, please providethefollowing. Web all appeals must be submitted in writing, using the aetna provider complaint and appeal form. How do i submit requests for reconsideration online? To obtain a review submit this form as. Web where should i send my dispute if.

Gallery of Aetna Provider Claim Resubmission Reconsideration form New
To obtain a review submit this form as. Web all appeals must be submitted in writing, using the aetna provider complaint and appeal form. Web claim reconsideration can be submitted if a claim does not require any changes, but a provider is not satisfied with the claim disposition and wishes to dispute the original. Within 180 calendar days of the.

Sample Insurance Appeal Letter for No Authorization Sample Templates
Web 4 rows timeframes for reconsiderations and appeals. Edit your appeals from aetna online type text, add images, blackout confidential details, add comments, highlights and more. Web provider info provider network files these links provides access to our aetna better health of texas provider directory xml files which can be downloaded by third parties and. Web forms for health care.
Aetna Appeal Form 20202022 Fill and Sign Printable Template Online
Within 180 calendar days of the initial claim decision. Aetna is the brand name used for products and services provided by one or more of the aetna group of companies, including aetna life insurance company and its. Web claims reconsideration & appeals form complete this form and return to aetna better health of texas for processing your request. Get a.
Aetna Network Deficiency Form Fill Out and Sign Printable PDF
Web claims reconsideration & appeals form complete this form and return to aetna better health of texas for processing your request. What if i use the provider complaint and appeal form to. Aetna is the brand name used for products and services provided by one or more of the aetna group of companies, including aetna life insurance company and its..
Web If You Have A Dispute Around A Payment You Would Have Received Under Original Medicare Please Send Your Dispute, Documentation Of What Original Medicare.
Web claims reconsideration & appeals form complete this form and return to aetna better health of texas for processing your request. Web provider appeals dispute & appeal process: Web 4 rows timeframes for reconsiderations and appeals. How do i submit requests for reconsideration online?
To Obtain A Review Submit This Form As.
Sign it in a few clicks draw your signature, type. Web appeals must be submitted by mail/fax, using the provider complaint and appeal form. Within 180 calendar days of the initial claim decision. Web reconsideration denial notification date(s) cpt/hcpc/service being disputed.
Get A Provider Complaint And Appeal Form (Pdf) To Facilitate Handling:
Be specific when completing the description of dispute and. Web all appeals must be submitted in writing, using the aetna provider complaint and appeal form. What if i use the provider complaint and appeal form to. Web forms for health care professionals find all the forms you need find forms and applications for health care professionals and patients, all in one place.
Explanation Of Your Request (Please Use Additional Pages If Necessary.) You May Mail.
Reconsideration denial notification date(s) cpt/hcpc/service being disputed. Web medical dental member’s first name member’s last name member’s birthdate (mm/dd/yyyy) tohelp usreviewand respond to your request, please providethefollowing. Completion of this form is mandatory. Web claim reconsideration can be submitted if a claim does not require any changes, but a provider is not satisfied with the claim disposition and wishes to dispute the original.